

The Relevance of a Physical Active Lifestyle and Physical Fitness on Immune Defense: Mitigating Disease Burden, With Focus on COVID-19 Consequences
- PMID: 33613573
- PMCID: PMC7892446
- DOI: 10.3389/fimmu.2021.587146
The Relevance of a Physical Active Lifestyle and Physical Fitness on Immune Defense: Mitigating Disease Burden, With Focus on COVID-19 Consequences
Abstract
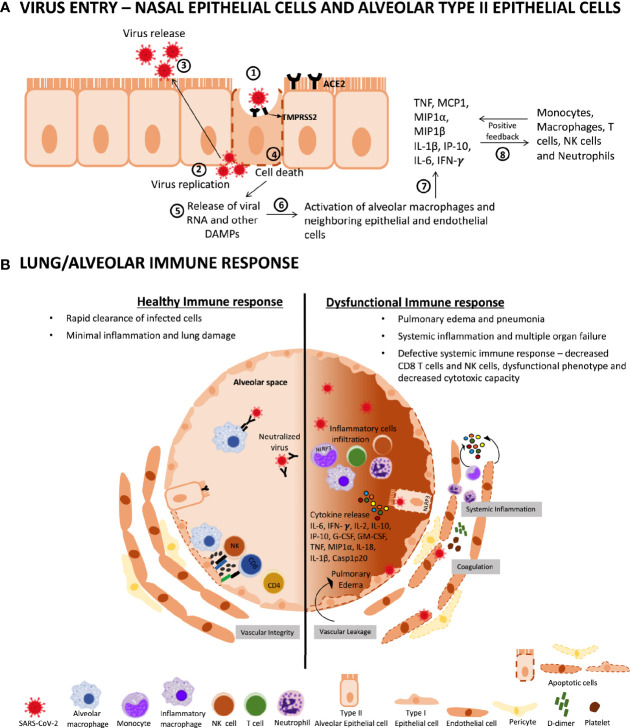
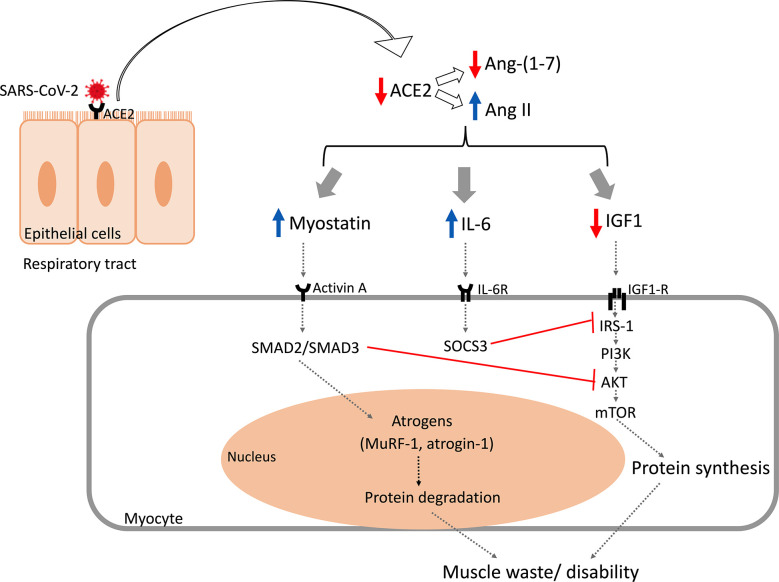
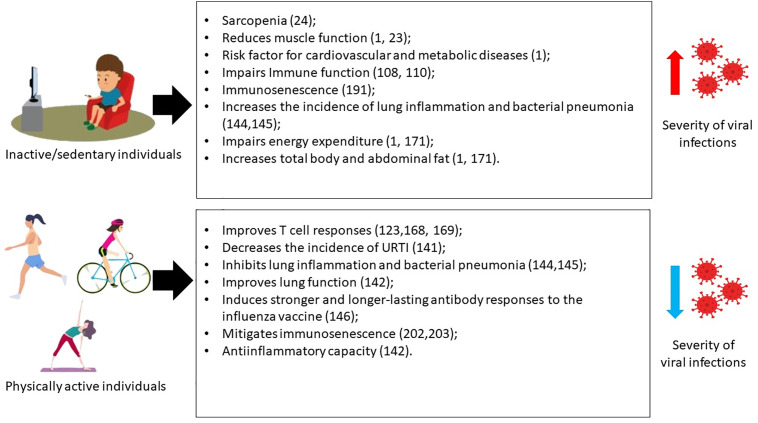
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is a fast spreading virus leading to the development of Coronavirus Disease-2019 (COVID-19). Severe and critical cases are characterized by damage to the respiratory system, endothelial inflammation, and multiple organ failure triggered by an excessive production of proinflammatory cytokines, culminating in the high number of deaths all over the world. Sedentarism induces worse, continuous, and progressive consequences to health. On the other hand, physical activity provides benefits to health and improves low-grade systemic inflammation. The aim of this review is to elucidate the effects of physical activity in physical fitness, immune defense, and its contribution to mitigate the severe inflammatory response mediated by SARS-CoV-2. Physical exercise is an effective therapeutic strategy to mitigate the consequences of SARS-CoV-2 infection. In this sense, studies have shown that acute physical exercise induces the production of myokines that are secreted in tissues and into the bloodstream, supporting its systemic modulatory effect. Therefore, maintaining physical activity influence balance the immune system and increases immune vigilance, and also might promote potent effects against the consequences of infectious diseases and chronic diseases associated with the development of severe forms of COVID-19. Protocols to maintain exercise practice are suggested and have been strongly established, such as home-based exercise (HBE) and outdoor-based exercise (OBE). In this regard, HBE might help to reduce levels of physical inactivity, bed rest, and sitting time, impacting on adherence to physical activity, promoting all the benefits related to exercise, and attracting patients in different stages of treatment for COVID-19. In parallel, OBE must improve health, but also prevent and mitigate COVID-19 severe outcomes in all populations. In conclusion, HBE or OBE models can be a potent strategy to mitigate the progress of infection, and a coadjutant therapy for COVID-19 at all ages and different chronic conditions.
Keywords: COVID-19; home-based exercise; immune system; sedentarism; social isolation.
Copyright © 2021 Filgueira, Castoldi, Santos, de Amorim, de Sousa Fernandes, Anastácio, Campos, Santos and Souto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Narici M, De Vito G, Franchi M, Paoli A, Moro T, Marcolin G, et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur J Sport Sci (2020), 1–22. 10.1080/17461391.2020.1761076 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous