

Effect of cannabis on oxaliplatin-induced peripheral neuropathy among oncology patients: a retrospective analysis
- PMID: 33613702
- PMCID: PMC7876573
- DOI: 10.1177/1758835921990203
Effect of cannabis on oxaliplatin-induced peripheral neuropathy among oncology patients: a retrospective analysis
Abstract
Background: Chemotherapy-induced peripheral neuropathy (CIPN) is a common and dosage-limited oxaliplatin-related toxicity. To date, there are no successful interventions for CIPN prevention or treatment. A therapeutic role for cannabis in diabetic and HIV-related peripheral neuropathy and a protective role in CIPN have been suggested. We examined the effect of cannabis on oncologic patients with CIPN.
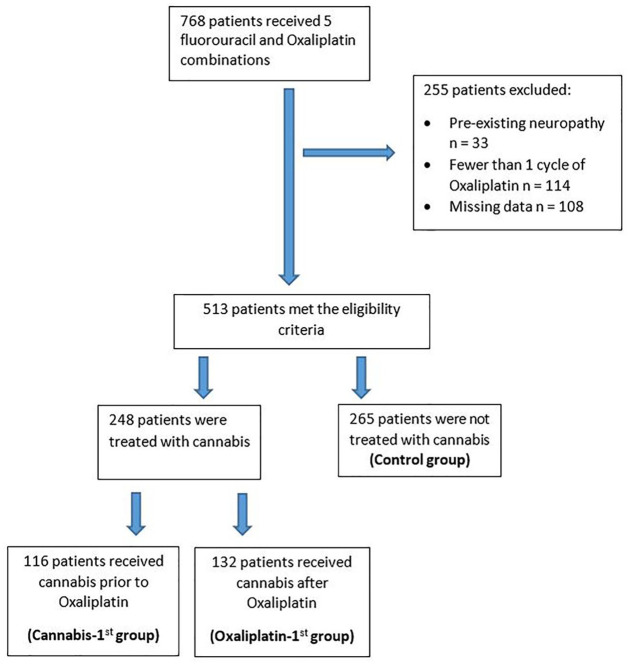
Methods: Medical records of 768 consecutive patients treated with oxaliplatin and 5-fluorouracil-based combinations at a tertiary medical center from October 2015 to January 2018 were reviewed. Excluded patients were those with pre-existing neuropathy or patients who received fewer than two cycles of oxaliplatin treatment. CIPN grade, oxaliplatin cumulative dose, and neuropathy-free survival were evaluated. The patients were divided based upon the exposure to cannabis: prior to oxaliplatin (cannabis-first), cannabis following the initiation of oxaliplatin treatment (oxaliplatin-first), and no exposure (control).
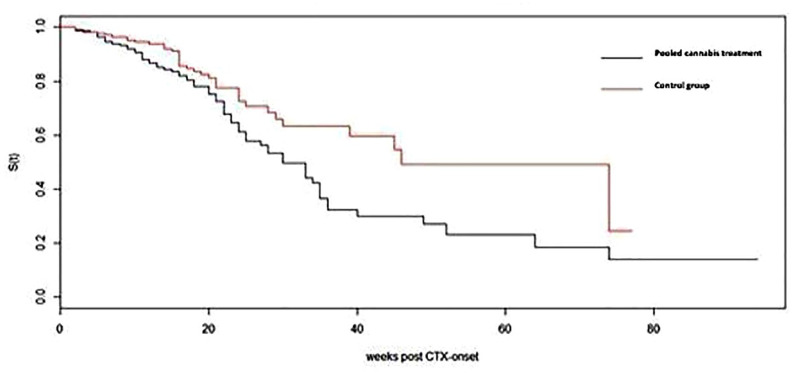
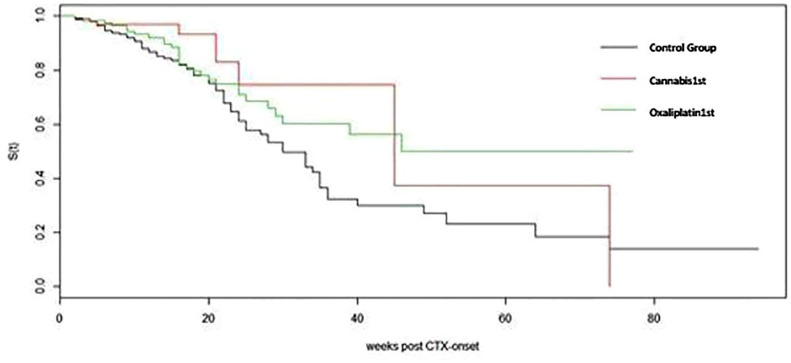
Results: In total, 513 patients met the inclusion criteria, of whom 248 were treated with cannabis and 265 served as controls. The cannabis-first group included 116 (46.7%) patients and the oxaliplatin-first group included 132 (53.3%) patients. Demographic parameters were comparable between groups. There was a significant difference in CIPN grade 2-3 between cannabis-exposed patients and controls (15.3% and 27.9%, respectively, p < 0.001). The protective effect of cannabis was more pronounced among cannabis-first patients compared to oxaliplatin-first patients (75% and 46.2%, respectively, p < 0.001). The median oxaliplatin cumulative doses were higher in the cannabis-first versus the oxaliplatin-first versus the control groups (545 mg/m2, 340 mg/m2, and 425 mg/m2 respectively, p < 0.001).
Conclusion: The rate of neuropathy was reduced among patients treated with cannabis and oxaliplatin. This reduction was more significant in patients who received cannabis prior to treatment with oxaliplatin, suggesting a protective effect. A large prospective trial is planned.
Keywords: cannabis; neuropathy; oxaliplatin; palliation; side effects.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: Barliz Waissengrin: no conflict of interest. Dan Mirelman: no conflict of interest. Sharon Pelles: no conflict of interest. Felix Bukstein: no conflict of interest. Deborah T. Blumenthal: medical advisor: VBL, ViruCure; honoraria: Takeda, AstraZeneca. Ido Wolf: honoraria: BMS; lectures/research grant: Novartis, BMS, Roche; consulting and advisory: Roche. Ravit Geva: options: BOL Pharma; honoraria: MSD, Novartis, BMS, Roche, Janssen, Medison, Lilly, Bayer, Pfizer; consulting and advisory: BOL Pharma, MSD, Bayer, Novartis, Boehringer Ingelheim; travel, accommodations, expenses: Bayer, Merck, Medison, BMS.
Figures
References
-
- André T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004; 23: 2343–2351. - PubMed
-
- André T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 2009; 19: 3109–3116. - PubMed
-
- de Gramont AD, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol 2000; 16: 2938–2947. - PubMed
-
- Rothenberg ML, Oza AM, Bigelow RH, et al. Superiority of oxaliplatin and fluorouracil-leucovorin compared with either therapy alone in patients with progressive colorectal cancer after irinotecan and fluorouracil-leucovorin: interim results of a phase III trial. J Clin Oncol 2003; 11: 2059–2069. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
