

Subcutaneous daratumumab and hyaluronidase-fihj in newly diagnosed or relapsed/refractory multiple myeloma
- PMID: 33613930
- PMCID: PMC7841854
- DOI: 10.1177/2040620720987075
Subcutaneous daratumumab and hyaluronidase-fihj in newly diagnosed or relapsed/refractory multiple myeloma
Abstract
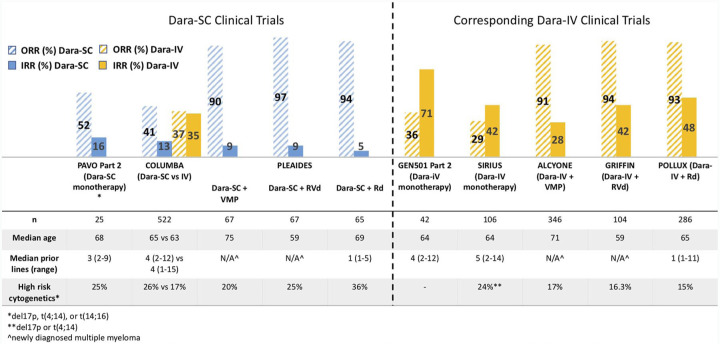
Daratumumab, a human immunoglobulin G1 kappa monoclonal antibody that targets CD38, is currently approved as monotherapy and in varying combinations with approved anti-myeloma regimens in both newly diagnosed multiple myeloma and relapsed refractory multiple myeloma. Originally developed for intravenous administration, the subcutaneous formulation of daratumumab (daratumumab and hyaluronidase-fihj) was recently approved by the US Federal Drug Administration and European Commission in 2020. In clinical trials, compared with the intravenous formulation, subcutaneous daratumumab (Dara-SC) has significantly shorter administration time (median first dose 7 h versus 3-5 min, respectively), lower rates of infusion-related reactions (median first dose 50% versus less than 10%, respectively), and lower volume of infusion (median 500-1000 ml versus 15 ml, respectively). Otherwise, the pharmacokinetics, safety profile, and efficacy are comparable. This review summarizes the pivotal trials that led to the approval of Dara-SC, highlights important clinical considerations for the use of Dara-SC, and provides practical guidelines for the administration of Dara-SC in the clinic.
Keywords: CD38; daratumumab; monoclonal antibody; multiple myeloma; myeloma; newly diagnosed; relapsed refractory; subcutaneous.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: LS: no relevant disclosures; JR: speaking fees from Celgene and Janssen, advisory board and consulting fees from Celgene, Janssen, Bristol Myers Squibb, Oncopeptides, Adaptive Biotechnologies, X4 Pharmaceuticals, Karyopharm, and Antegene; HJC: employed by the Multiple Myeloma Research Foundation, advisory board and consulting fees from Genetech, Celgene, Bristol Myers Squibb, GlaxoSmithKline and received research funding from Takeda, Celgene, and Genetech; SJ: advisory board and consulting fees from Celgene, Bristol Myers Squibb, Janssen Pharmaceuticals and Merck; DM: advisory board and consulting fees from Janssen, Celgene, Bristol Myers Squibb, Takeda, Legend, GlaxoSmithKline, Kinevant, and Foundation Medicine; SP: consulting fees from Foundation Medicine, research funding from Celgene and Karyopharm; SR: no relevant disclosures; LT: no relevant disclosures; DV: no relevant disclosures; AC: advisory board and consulting fees from Amgen, Antegene, Celgene, Janssen, Karyopharm, Millennium/Takeda, Novartis Pharmaceuticals, Oncopeptides, Sanofi; research funding from Amgen, Celgene, Janssen, Millennium/Takeda, Novartis Pharmaceuticals, Pharmacyclics.
Figures
References
-
- Lonial S, Weiss BM, Usmani SZ, et al. Daratumumab monotherapy in patients with treatment-refractory multiple myeloma (SIRIUS): an open-label, randomised, phase 2 trial. Lancet 2016; 387: 1551–1560. - PubMed
-
- Lokhorst HM, Plesner T, Laubach JP, et al. Targeting CD38 with daratumumab monotherapy in multiple myeloma. N Engl J Med 2015; 373: 1207–1219. - PubMed
-
- Palumbo A, Chanan-Khan A, Weisel K, et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375: 754–766. - PubMed
-
- Dimopoulos MA, Oriol A, Nahi H, et al. Daratumumab, lenalidomide, and dexamethasone for multiple myeloma. N Engl J Med 2016; 375: 1319–1331. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
