

Measurable Residual Disease Assessed by Flow-Cytometry Is a Stable Prognostic Factor for Pediatric T-Cell Acute Lymphoblastic Leukemia in Consecutive SEHOP Protocols Whereas the Impact of Oncogenetics Depends on Treatment
- PMID: 33614543
- PMCID: PMC7892614
- DOI: 10.3389/fped.2020.614521
Measurable Residual Disease Assessed by Flow-Cytometry Is a Stable Prognostic Factor for Pediatric T-Cell Acute Lymphoblastic Leukemia in Consecutive SEHOP Protocols Whereas the Impact of Oncogenetics Depends on Treatment
Abstract
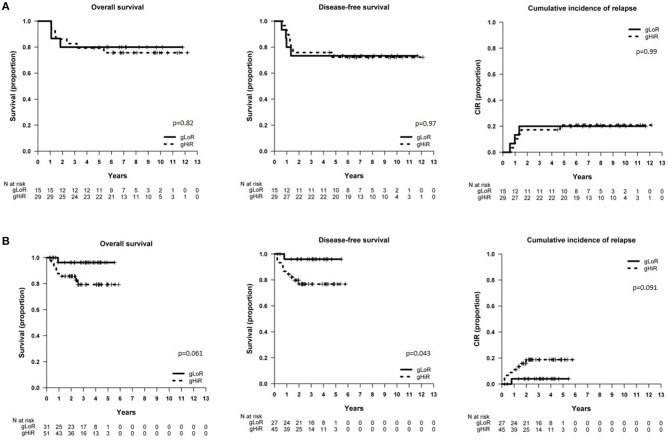
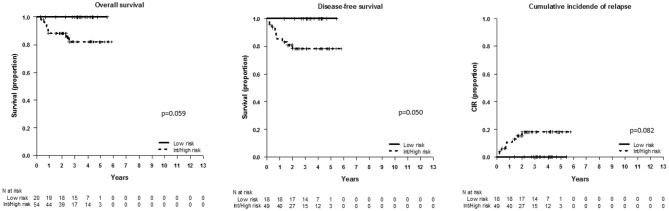
Robust and applicable risk-stratifying genetic factors at diagnosis in pediatric T-cell acute lymphoblastic leukemia (T-ALL) are still lacking, and most protocols rely on measurable residual disease (MRD) assessment. In our study, we aimed to analyze the impact of NOTCH1, FBXW7, PTEN, and RAS mutations, the measurable residual disease (MRD) levels assessed by flow cytometry (FCM-MRD) and other reported risk factors in a Spanish cohort of pediatric T-ALL patients. We included 199 patients treated with SEHOP and PETHEMA consecutive protocols from 1998 to 2019. We observed a better outcome of patients included in the newest SEHOP-PETHEMA-2013 protocol compared to the previous SHOP-2005 cohort. FCM-MRD significantly predicted outcome in both protocols, but the impact at early and late time points differed between protocols. The impact of FCM-MRD at late time points was more evident in SEHOP-PETHEMA 2013, whereas in SHOP-2005 FCM-MRD was predictive of outcome at early time points. Genetics impact was different in SHOP-2005 and SEHOP-PETHEMA-2013 cohorts: NOTCH1 mutations impacted on overall survival only in the SEHOP-PETHEMA-2013 cohort, whereas homozygous deletions of CDKN2A/B had a significantly higher CIR in SHOP-2005 patients. We applied the clinical classification combining oncogenetics, WBC count and MRD levels at the end of induction as previously reported by the FRALLE group. Using this score, we identified different subgroups of patients with statistically different outcome in both Spanish cohorts. In SHOP-2005, the FRALLE classifier identified a subgroup of high-risk patients with poorer survival. In the newest protocol SEHOP-PETHEMA-2013, a very low-risk group of patients with excellent outcome and no relapses was detected, with borderline significance. Overall, FCM-MRD, WBC count and oncogenetics may refine the risk-stratification, helping to design tailored approaches for pediatric T-ALL patients.
Keywords: NOTCH1; T-cell acute lymphoblastic leukemia; flow cytometry; measurable (minimal) residual disease; oncogenetics; pediatrics; risk-factors.
Copyright © 2021 Vega-García, Perez-Jaume, Esperanza-Cebollada, Vicente-Garcés, Torrebadell, Jiménez-Velasco, Ortega, Llop, Abad, Vagace, Minguela, Pratcorona, Sánchez-Garcia, García-Calderón, Gómez-Casares, Martín-Clavero, Escudero, Riñón Martinez-Gallo, Muñoz, Velasco, García-Morin, Català, Pascual, Velasco, Fernández, Lassaletta, Fuster, Badell, Molinos-Quintana, Molinés, Guerra-García, Pérez-Martínez, García-Abós, Robles Ortiz, Pisa, Adán, Díaz de Heredia, Dapena, Rives, Ramírez-Orellana, Camós and on behalf of the Biological Committee of the Group of Leukaemia of the Spanish Society of Paediatric Haematology Oncology (SEHOP Group).
Conflict of interest statement
MT reports travel and accommodation support from Novartis (outside the submitted work); travel and accommodation support from Jazz Pharma and Shire/Servier (outside the submitted work); and travel and accommodation support from Amgen (outside the submitted work). JLF is a consultant/advisory member for Amgen, Jazz Pharmaceuticals, and Novartis (outside the submitted work), receives honoraria for speaking at symposia from Amgen, Servier, Jazz Pharmaceuticals, and Pfizer (outside the submitted work) and support for attending symposia from Servier and Jazz Pharmaceuticals (outside the submitted work). AM discloses talk fees from Jazz Pharma and Shire/Servier outside the presented work and reports travel and accommodation support from Jazz Pharma, Shire/Servier, and Novartis (outside the submitted work). JD reports advisory board honorarium, speaker fees, and travel and accommodation support from Jazz Pharma and Shire/Servier; personal fees, advisory board honorarium, speaker fees, and travel and accommodation support from Novartis (outside the submitted work); advisory board honorarium, and travel and accommodation support from Amgen (outside the submitted work); advisory board honorarium, speaker fees, and travel and accommodation support from Celgene (outside the submitted work); advisory board honorarium, speaker fees, and travel and accommodation support from Sobi (outside the submitted work). SR reports advisory board honorarium, speaker fees, and travel and accommodation support from Jazz Pharma and Shire/Servier; personal fees, advisory board honorarium, speaker fees, and travel and accommodation support from Novartis (outside the submitted work); advisory board honorarium, and travel and accommodation support from Amgen (outside the submitted work); advisory board honorarium, speaker fees, and travel and accommodation support from Celgene (outside the submitted work). MC discloses talk fees from Shire/Servier outside the presented work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Rives S, Estella J, Camós M, García-Miguel P, Verdeguer A, Couselo JM, et al. . [T-cell pediatric acute lymphoblastic leukemia: analysis of survival and prognostic factors in 4 consecutive protocols of the Spanish cooperative study group SHOP]. Med Clin. (2012) 139:141–9. 10.1016/j.medcli.2011.12.019 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous