

Severity of Intrarenal Arterial Lesions Can Predict the Clinical Prognosis of Hepatitis B Virus-Associated Glomerulonephritis: A Retrospective Study
- PMID: 33614735
- PMCID: PMC7879251
- DOI: 10.1159/000509088
Severity of Intrarenal Arterial Lesions Can Predict the Clinical Prognosis of Hepatitis B Virus-Associated Glomerulonephritis: A Retrospective Study
Abstract
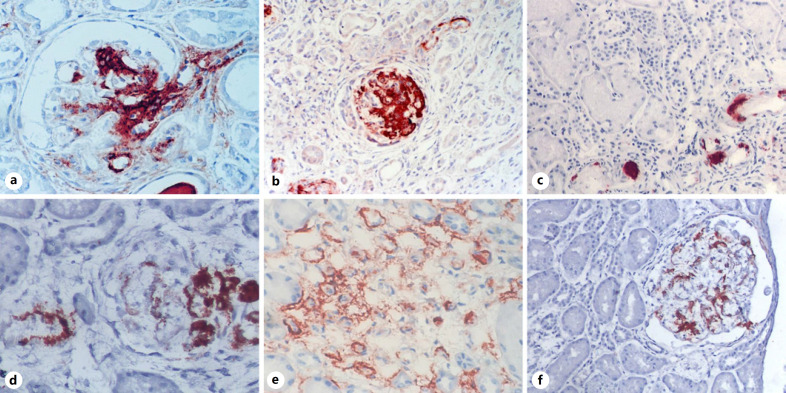
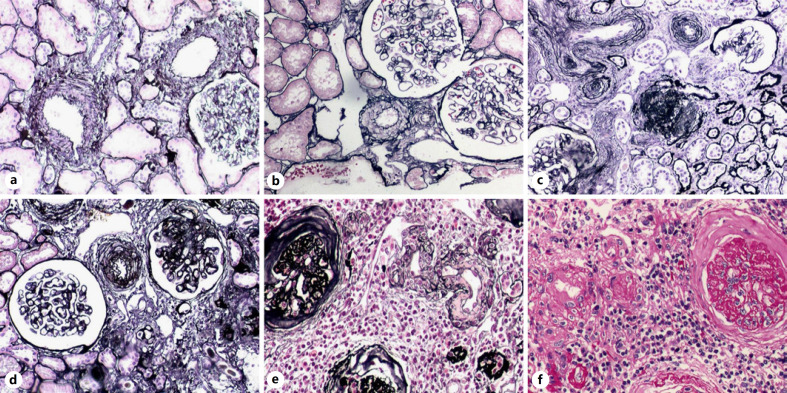
Background: Intrarenal arterial lesions (IALs) have been studied in immunoglobulin A nephropathy and lupus nephritis, but this has not been reported in hepatitis B virus-associated glomerulonephritis (HBV-GN). This study aims to investigate the prevalence and the role of IALs in HBV-GN.
Methods: IALs were examined in kidney biopsy specimens from 205 patients with HBV-GN retrospectively. The severity of IALs and tubular interstitial lesions was scored semi-quantitatively. The severity of IALs was divided into 4 groups on the basis of ILA score, which were no IALs (Score 0), mild IALs (Score 1-2), moderate IALs (Score 3-4), and severe IALs (Score 5-10) groups. Survival analysis was performed using the Kaplan-Meier method between the severity of IALs and clinical events (doubling of serum creatinine [SCr], ESRD, and death due to the kidney disease).
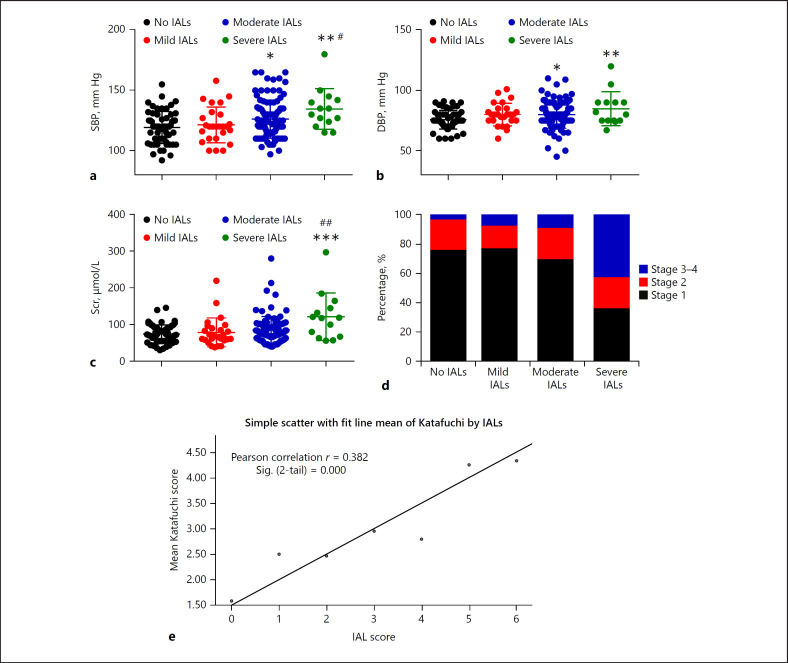
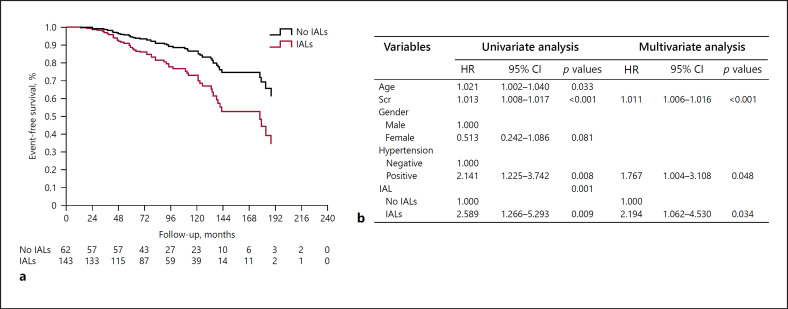
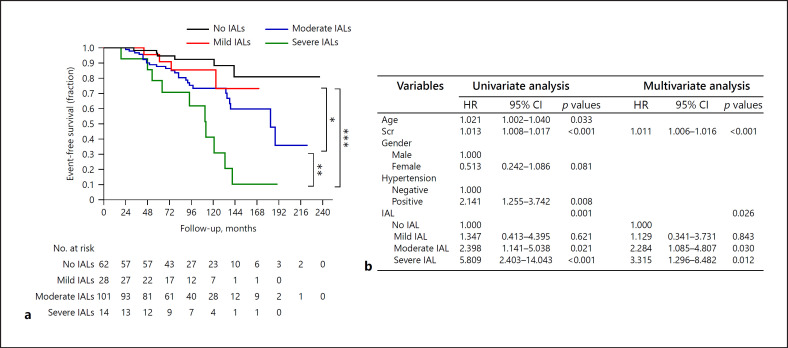
Results: Among 205 patients with HBV-GN, 143 (69.8%) had IALs in their kidney biopsy specimens. IALs were mild in 28 (19.6%) patients, moderate in 101 (70.6%) patients, and severe in 14 (9.8%) patients. The severity of IALs was associated with high blood pressure (BP), high SCr, and severe tubulointerstitial injuries. The average follow-up time of these 205 HBV-GN patients was 94.2 ± 47.1 months, in which 46 cases had clinical event. The proportions of clinical events in no IAL, mild IAL, moderate IAL, and severe IAL groups were 9.7, 14.3, 25.7, and 71.4%, respectively. Event-free survival of patient in IAL group was significantly lower than that in the no IAL group (p = 0.000). Multivariate cox regression analysis indicated SCr (1.011, 1.007-1.016), hypertension (1.767, 1.004-3.108), and IAL (2.194, 1.062-4.530) were independent risk factors for clinical events after adjustment for age and gender. Event-free clinical survival in moderate and severe IAL groups was significantly lower than that in the no IAL group (p = 0.0111 and p = 0.0001, respectively). Besides, event-free renal survival in severe IAL group was significantly lower than that in moderate IAL group (p = 0.009). Multivariate cox regression analysis showed that the more severe the IALs, the higher the risk of the clinical event, with a hazard ratio of 2.284 for moderate IALs (1.085-4.907) and 3.315 for severe IALs (1.296-8.482).
Conclusions: Severity of IALs is associated with high BP, reduced renal function, and poor clinical prognosis in HBV-GN patients.
Keywords: Hepatitis B virus-associated glomerulonephritis; Intrarenal arterial lesion; Renal biopsy; Tubular interstitial injury.
Copyright © 2020 by S. Karger AG, Basel.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
Similar articles
-
Impact of intrarenal arterial lesions on prognosis of IgA nephropathy: insights from a retrospective cohort study.Ren Fail. 2025 Dec;47(1):2476052. doi: 10.1080/0886022X.2025.2476052. Epub 2025 Mar 12. Ren Fail. 2025. PMID: 40074703 Free PMC article.
-
Impaired perfusion in the myocardial microcirculation in asymptomatic patients with Stages 1-4 chronic kidney disease with intrarenal arterial lesions.Nephrol Dial Transplant. 2021 Nov 9;36(11):2066-2075. doi: 10.1093/ndt/gfaa245. Nephrol Dial Transplant. 2021. PMID: 33877359
-
Study on hyperuricemia in HBV-associated glomerulonephritis.Am J Clin Pathol. 2014 Jan;141(1):72-7. doi: 10.1309/AJCP2H0FOVIRWMSU. Am J Clin Pathol. 2014. PMID: 24343739
-
Meta-analysis of combined therapy for adult hepatitis B virus-associated glomerulonephritis.World J Gastroenterol. 2012 Feb 28;18(8):821-32. doi: 10.3748/wjg.v18.i8.821. World J Gastroenterol. 2012. PMID: 22371643 Free PMC article. Review.
-
Meta-analysis of the efficacy and safety of nucleotide/nucleoside analog monotherapy for hepatitis B virus-associated glomerulonephritis.Clin Nephrol. 2016 Jan;85(1):21-9. doi: 10.5414/CN108648. Clin Nephrol. 2016. PMID: 26636326 Review.
Cited by
-
Targeting hepatitis B virus-associated nephropathy: efficacy and challenges of current antiviral treatments.Clin Exp Med. 2025 Feb 15;25(1):57. doi: 10.1007/s10238-025-01584-4. Clin Exp Med. 2025. PMID: 39954162 Free PMC article. Review.
-
Clinicopathologic features and long-term prognosis of hepatitis B virus-associated glomerulonephritis: a retrospective cohort study.J Nephrol. 2023 Nov;36(8):2335-2344. doi: 10.1007/s40620-023-01685-x. Epub 2023 Jul 31. J Nephrol. 2023. PMID: 37523106 Free PMC article.
References
-
- Zhuang Y, Yu Y, Huang Y, Zhong X. Study on hyperuricemia in HBV-associated glomerulonephritis. Am J Clin Pathol. 2014;141((1)):72–7. - PubMed
-
- Bhimma R, Coovadia HM, Adhikari M. Hepatitis B virus-associated nephropathy in black South African children. Pediatr Nephrol. 2004;12((6)):479–84. - PubMed
-
- Xu G, Huang T. Hepatitis B virus-associated glomerular nephritis in East Asia: progress and challenges. Eur J Intern Med. 2011;22((2)):161–6. - PubMed
-
- Khedmat H, Taheri S. Hepatitis B virus-associated nephropathy: an International Data Analysis. Iran J Kidney Dis. 2010;4((2)):101–5. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
