

Although Surgical Techniques Differ, Similar Outcomes Can Be Obtained When Operating After Single Versus Multiple Anterior Shoulder Dislocations
- PMID: 33615260
- PMCID: PMC7879183
- DOI: 10.1016/j.asmr.2020.09.006
Although Surgical Techniques Differ, Similar Outcomes Can Be Obtained When Operating After Single Versus Multiple Anterior Shoulder Dislocations
Abstract
Purpose: To compare the differences in preoperative pathology, surgical technique, and overall outcomes between patients treated surgically after a single anterior glenohumeral joint dislocation and those undergoing surgery after multiple dislocations.
Methods: An epidemiologic database was used to identify all patients younger than 40 years undergoing surgery for anterior shoulder instability between January 1, 1994, and July 31, 2016, in a defined geographic area. Patient medical records were reviewed to obtain demographic information, patient history, physical examination findings, imaging findings, clinical progression, surgical details, and outcomes. Comparative analysis was performed between patients who underwent surgery after a single dislocation and those who underwent surgery after multiple preoperative dislocations.
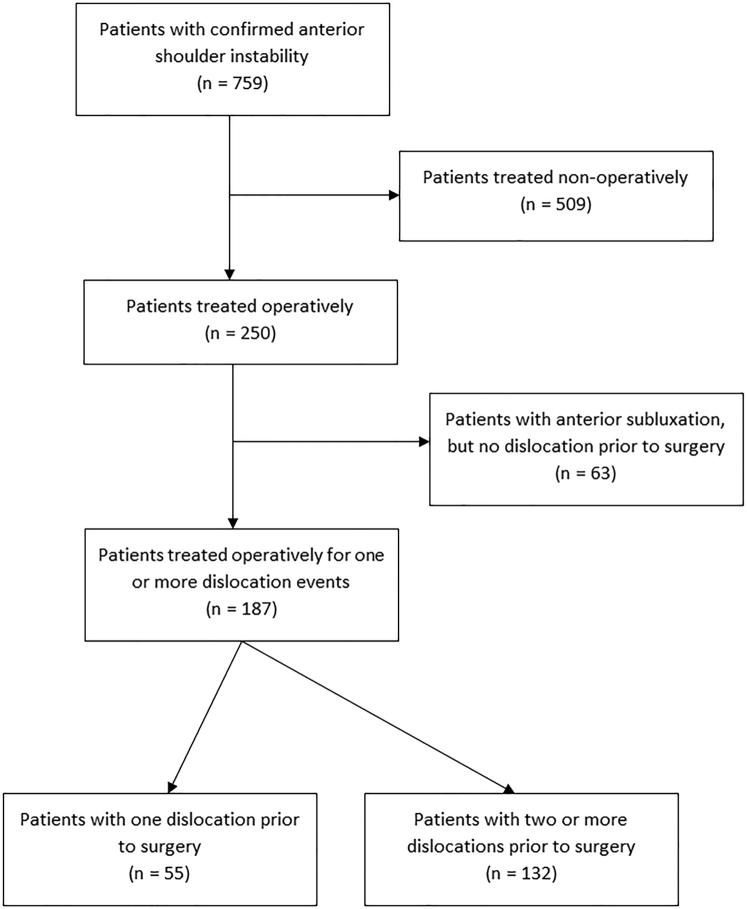
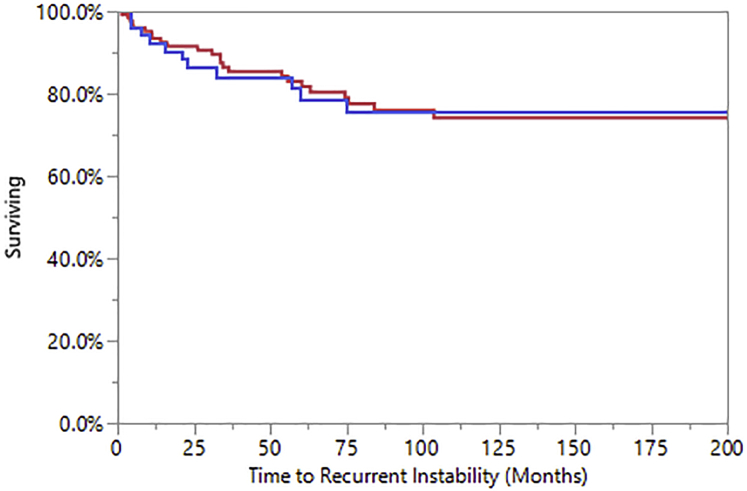
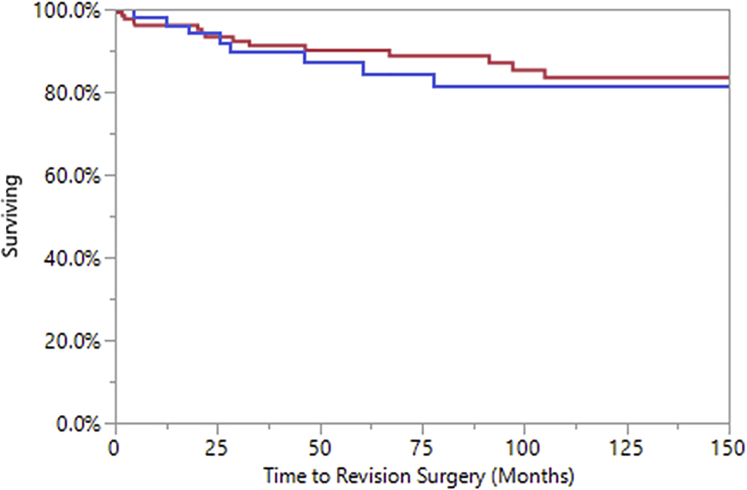
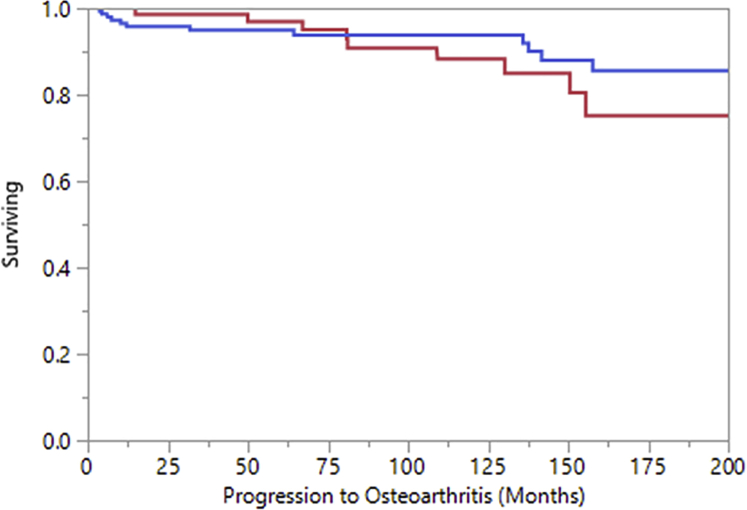
Results: The study population consisted of 187 patients who had a single anterior shoulder dislocation (n = 55) or multiple anterior shoulder dislocations (n = 132) prior to surgery. The mean follow-up period was 103.3 months (range, 0.3-328.4 months). Demographic characteristics were not significantly different between groups. Although the presence of Hill-Sachs lesions on radiographs was more common in the multiple-dislocation group (42.1%) than in the single-dislocation group (18.8%, P = .005), there were no other significant differences in concomitant pathology between groups. Latarjet procedures were more commonly performed in the multiple-dislocation group (12.5% vs 2.1% in the single-dislocation group, P = .04). There were no other significant differences in surgical techniques and characteristics between groups. Rates of survival free from recurrent instability (P = .790), revision surgery (P = .726), and progression to symptomatic osteoarthritis (P = .588) were not significantly different between groups.
Conclusions: Although patients with multiple dislocations prior to surgery were more likely to show radiographic evidence of Hill-Sachs lesions and undergo the Latarjet procedure than those who received surgery after a single dislocation, no significant differences in outcomes with respect to recurrent instability, revision surgery, or progression to symptomatic osteoarthritis were found between these 2 groups at long-term follow-up.
Level of evidence: Level III, retrospective comparative study.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier Inc.
Figures
Similar articles
-
Clinical and Anatomic Predictors of Outcomes After the Latarjet Procedure for the Treatment of Anterior Glenohumeral Instability With Combined Glenoid and Humeral Bone Defects.Am J Sports Med. 2016 Jun;44(6):1407-16. doi: 10.1177/0363546516634089. Epub 2016 Mar 29. Am J Sports Med. 2016. PMID: 27217523
-
Remplissage Versus Modified Latarjet for Off-Track Hill-Sachs Lesions With Subcritical Glenoid Bone Loss.Am J Sports Med. 2018 Jul;46(8):1885-1891. doi: 10.1177/0363546518767850. Epub 2018 Apr 19. Am J Sports Med. 2018. PMID: 29672132
-
Recurrent Anterior Shoulder Instability With Combined Bone Loss: Treatment and Results With the Modified Latarjet Procedure.Am J Sports Med. 2016 Apr;44(4):922-32. doi: 10.1177/0363546515623929. Epub 2016 Feb 1. Am J Sports Med. 2016. PMID: 26831633
-
Outcomes of the Latarjet Procedure Versus Free Bone Block Procedures for Anterior Shoulder Instability: A Systematic Review and Meta-analysis.Am J Sports Med. 2021 Mar;49(3):805-816. doi: 10.1177/0363546520925833. Epub 2020 Aug 14. Am J Sports Med. 2021. PMID: 32795174
-
Surgical stabilization of pediatric anterior shoulder instability yields high recurrence rates: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2021 Jan;29(1):192-201. doi: 10.1007/s00167-020-05913-w. Epub 2020 Feb 28. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32112125
Cited by
-
Artificial Intelligence Can Define and Predict the "Optimal Observed Outcome" After Anterior Shoulder Instability Surgery: An Analysis of 200 Patients With 11-Year Mean Follow-Up.Arthrosc Sports Med Rehabil. 2023 Jul 22;5(4):100773. doi: 10.1016/j.asmr.2023.100773. eCollection 2023 Aug. Arthrosc Sports Med Rehabil. 2023. PMID: 37520500 Free PMC article.
-
Single anterior shoulder dislocation patients demonstrate higher rates of posterior labral repair and biceps procedures than multiple dislocators at the time of arthroscopic stabilization surgery.JSES Int. 2024 Jul 3;8(5):978-983. doi: 10.1016/j.jseint.2024.06.008. eCollection 2024 Sep. JSES Int. 2024. PMID: 39280167 Free PMC article.
References
-
- Chan A.G., Kilcoyne K.G., Chan S., Dickens J.F., Waterman B.R. Evaluation of the Instability Severity Index score in predicting failure following arthroscopic Bankart surgery in an active military population. J Shoulder Elbow Surg. 2019;28:e156–e163. - PubMed
-
- Hong J., Huang Y., Ma C., et al. Risk factors for anterior shoulder instability: A matched case-control study. J Shoulder Elbow Surg. 2019;28:869–874. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
