

Biventricular function in exercise during autonomic (thoracic epidural) block
- PMID: 33615388
- PMCID: PMC8064994
- DOI: 10.1007/s00421-021-04631-6
Biventricular function in exercise during autonomic (thoracic epidural) block
Abstract
Background: Blockade of cardiac sympathetic fibers by thoracic epidural anesthesia (TEA) was previously shown to reduce right and left ventricular systolic function and effective pulmonary arterial elastance. At conditions of constant paced heart rate, cardiac output and systemic hemodynamics were unchanged. In this study, we further investigated the effect of cardiac sympathicolysis during physical stress and increased oxygen demand.
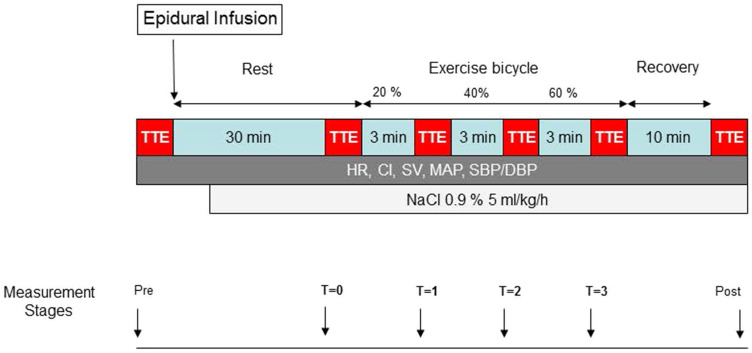
Methods: In a cross-over design, 12 patients scheduled to undergo thoracic surgery performed dynamic ergometric exercise tests with and without TEA. Hemodynamics were monitored and biventricular function was measured by transthoracic two-dimensional and M-mode echocardiography, pulsed wave Doppler and tissue Doppler imaging.
Results: TEA attenuated systolic RV function (TV S': - 21%, P < 0.001) and LV function (MV S': - 14%, P = 0.025), but biventricular diastolic function was not affected. HR (- 11%, P < 0.001), SVI (- 15%, P = 0.006), CI (- 21%, P < 0.001) and MAP (- 12%, P < 0.001) were decreased during TEA, but SVR was not affected. Exercise resulted in significant augmentation of systolic and diastolic biventricular function. During exercise HR, SVI, CI and MAP increased (respectively, + 86%, + 19%, + 124% and + 17%, all P < 0.001), whereas SVR decreased (- 49%, P < 0.001). No significant interactions between exercise and TEA were found, except for RPP (P = 0.024) and MV E DT (P = 0.035).
Conclusion: Cardiac sympathetic blockade by TEA reduced LV and RV systolic function but did not significantly blunt exercise-induced increases in LV and RV function. These data indicate that additional mechanisms besides those controlled by the cardiac sympathetic nervous system are involved in the regulation of cardiac function during dynamic exercise. Trial registration Clinical trial registration: Nederlands Trial Register, NTR 4880 http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=4880 .
Keywords: Anesthesia; Autonomic; Circulation; Epidural; Exercise; Nervous system; Ventricular function, left; Ventricular function, right.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Bates D, Mächler M, Bolker B, Walker S. Fitting linear mixed-effects models usinglme4. J Stat Softw. 2015 doi: 10.18637/jss.v067.i01. - DOI
-
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc. 1995;57:289–300.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
