

Sensitive and Feasible Specimen Collection and Testing Strategies for Diagnosing Tuberculosis in Young Children
- PMID: 33616611
- PMCID: PMC7900937
- DOI: 10.1001/jamapediatrics.2020.6069
Sensitive and Feasible Specimen Collection and Testing Strategies for Diagnosing Tuberculosis in Young Children
Abstract
Importance: Criterion-standard specimens for tuberculosis diagnosis in young children, gastric aspirate (GA) and induced sputum, are invasive and rarely collected in resource-limited settings. A far less invasive approach to tuberculosis diagnostic testing in children younger than 5 years as sensitive as current reference standards is important to identify.
Objective: To characterize the sensitivity of preferably minimally invasive specimen and assay combinations relative to maximum observed yield from all specimens and assays combined.
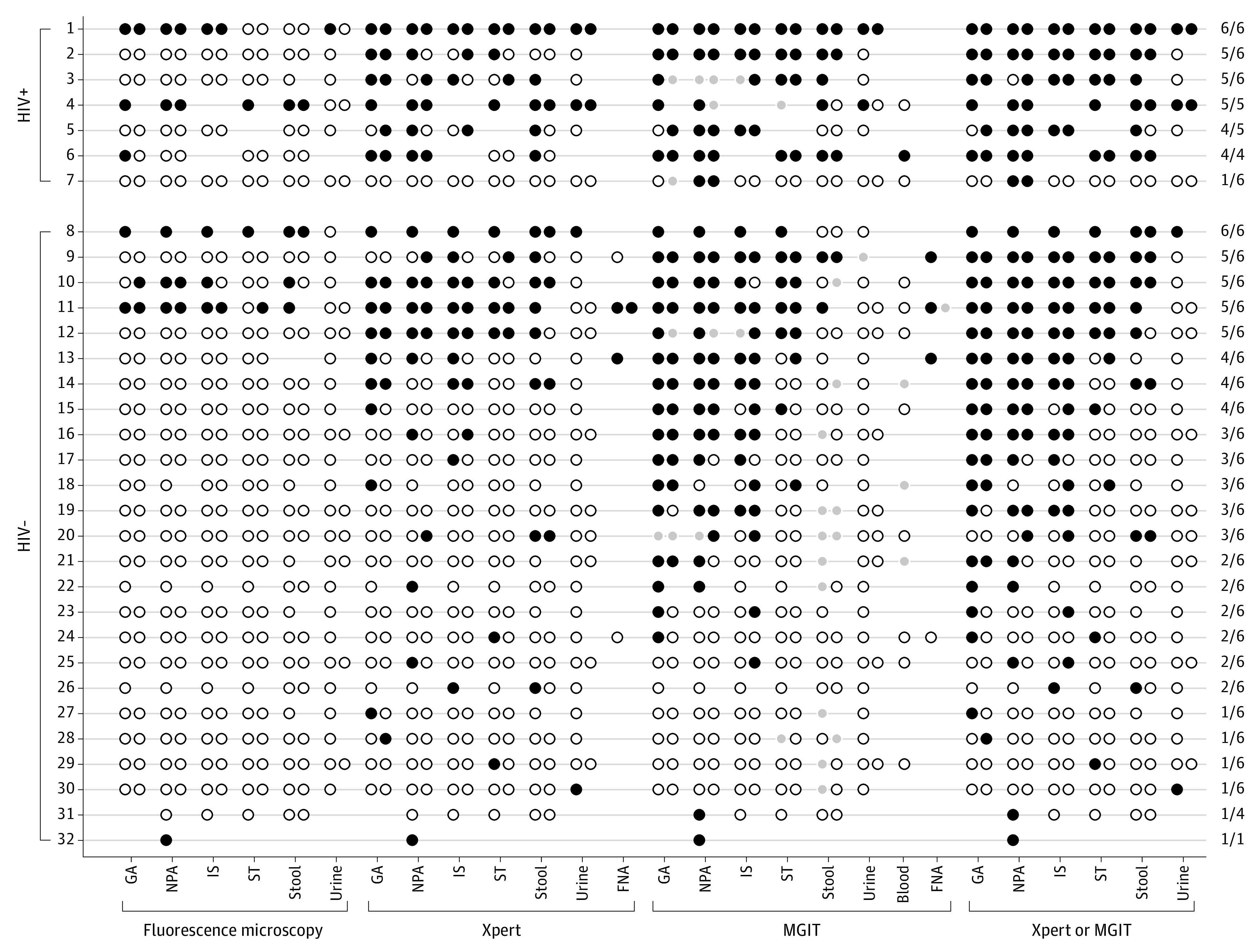
Design, setting, and participants: In this prospective cross-sectional diagnostic study, the reference standard was a panel of up to 2 samples of each of 6 specimen types tested for Mycobacterium tuberculosis complex by Xpert MTB/RIF assay and mycobacteria growth indicator tube culture. Multiple different combinations of specimens and tests were evaluated as index tests. A consecutive series of children was recruited from inpatient and outpatient settings in Kisumu County, Kenya, between October 2013 and August 2015. Participants were children younger than 5 years who had symptoms of tuberculosis (unexplained cough, fever, malnutrition) and parenchymal abnormality on chest radiography or who had cervical lymphadenopathy. Children with 1 or more evaluable specimen for 4 or more primary study specimen types were included in the analysis. Data were analyzed from February 2015 to October 2020.
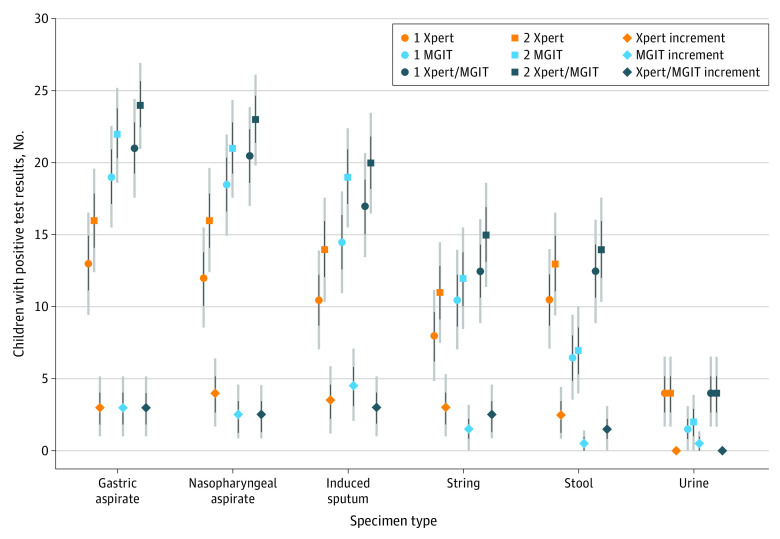
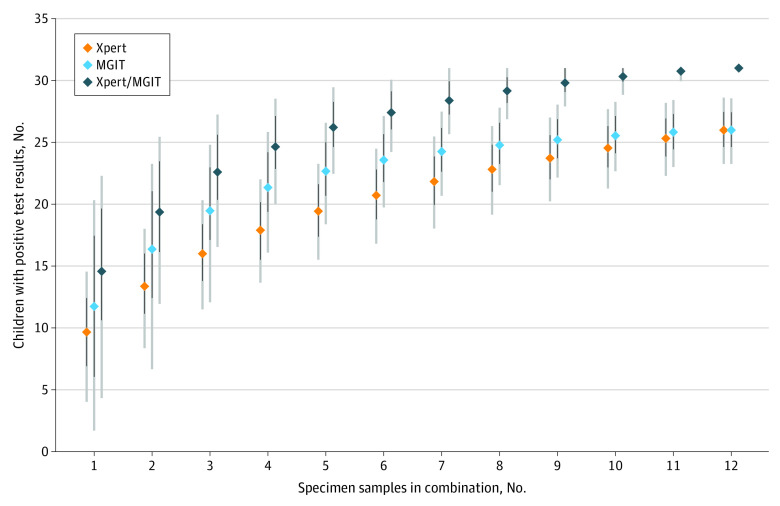
Main outcomes and measures: Cumulative and incremental diagnostic yield of combinations of specimen types and tests relative to the maximum observed yield.
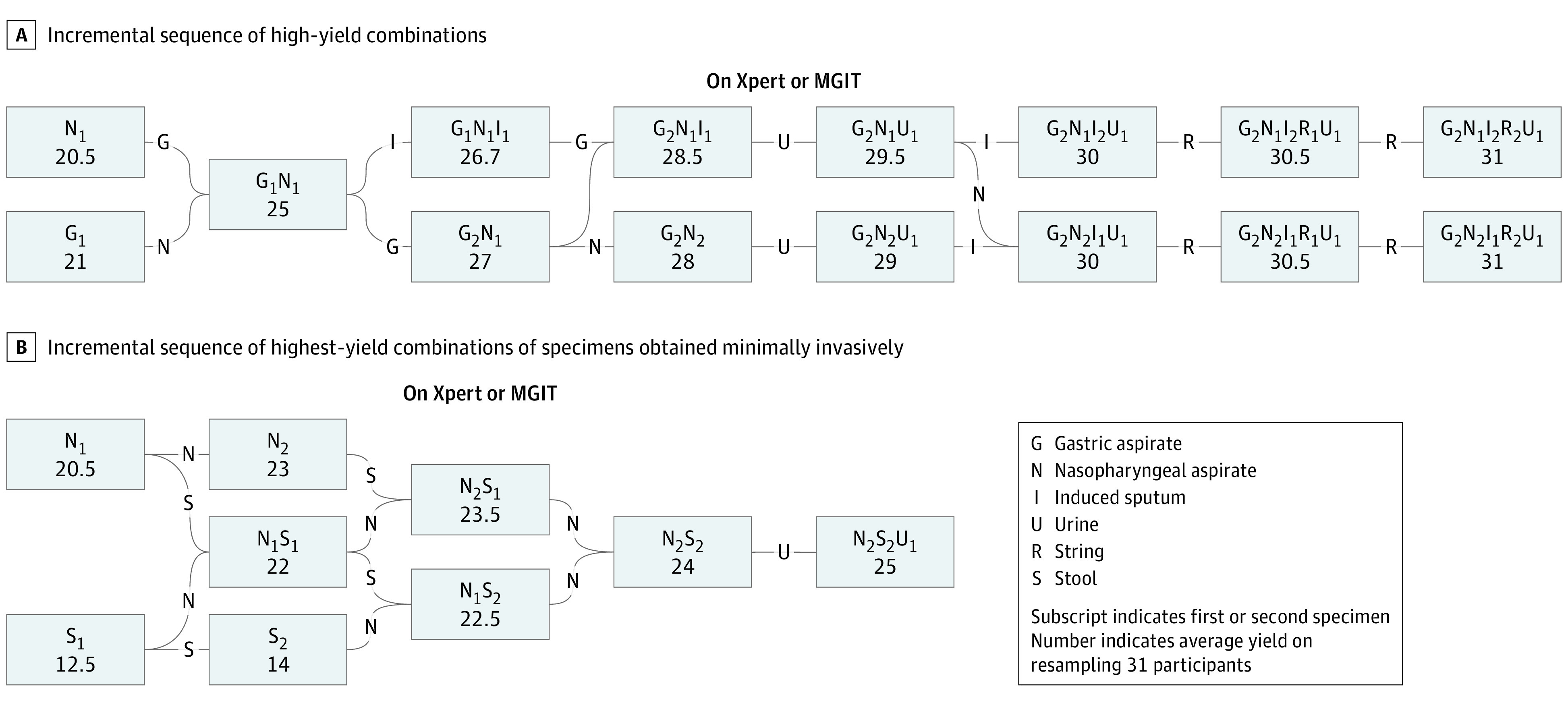
Results: Of the 300 enrolled children, the median (interquartile range) age was 2.0 (1.0-3.6) years, and 151 (50.3%) were female. A total of 294 met criteria for analysis. Of 31 participants with confirmed tuberculosis (maximum observed yield), 24 (sensitivity, 77%; interdecile range, 68%-87%) had positive results on up to 2 GA samples and 20 (sensitivity, 64%; interdecile range, 53%-76%) had positive test results on up to 2 induced sputum samples. The yields of 2 nasopharyngeal aspirate (NPA) samples (23 of 31 [sensitivity, 74%; interdecile range, 64%-84%]), of 1 NPA sample and 1 stool sample (22 of 31 [sensitivity, 71%; interdecile range, 60%-81%]), or of 1 NPA sample and 1 urine sample (21.5 of 31 [sensitivity, 69%; interdecile range, 58%-80%]) were similar to reference-standard specimens. Combining up to 2 each of GA and NPA samples had an average yield of 90% (28 of 31).
Conclusions and relevance: NPA, in duplicate or in combination with stool or urine specimens, was readily obtainable and had diagnostic yield comparable with reference-standard specimens. This combination could improve tuberculosis diagnosis among children in resource-limited settings. Combining GA and NPA had greater yield than that of the current reference standards and may be useful in certain clinical and research settings.
Conflict of interest statement
Figures
Comment in
-
Diagnosing Childhood Tuberculosis: A Small Step Forward.JAMA Pediatr. 2021 May 1;175(5):e206078. doi: 10.1001/jamapediatrics.2020.6078. Epub 2021 May 3. JAMA Pediatr. 2021. PMID: 33616639 No abstract available.
References
-
- World Health Organization . Global tuberculosis report 2020. Accessed January 13, 2021. https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-en...
-
- Marais BJ, Gie RP, Schaaf HS, et al. . The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis. 2004;8(4):392-402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
