

PREVENT: A Randomized, Placebo-controlled Crossover Trial of Avexitide for Treatment of Postbariatric Hypoglycemia
- PMID: 33616643
- PMCID: PMC8277203
- DOI: 10.1210/clinem/dgab103
PREVENT: A Randomized, Placebo-controlled Crossover Trial of Avexitide for Treatment of Postbariatric Hypoglycemia
Abstract
Context: Postbariatric hypoglycemia (PBH), characterized by enteroinsular axis overstimulation and hyperinsulinemic hypoglycemia, is a complication of bariatric surgery for which there is no approved therapy.
Objective: To evaluate efficacy and safety of avexitide [exendin (9-39)], a glucagon-like peptide-1 antagonist, for treatment of PBH.
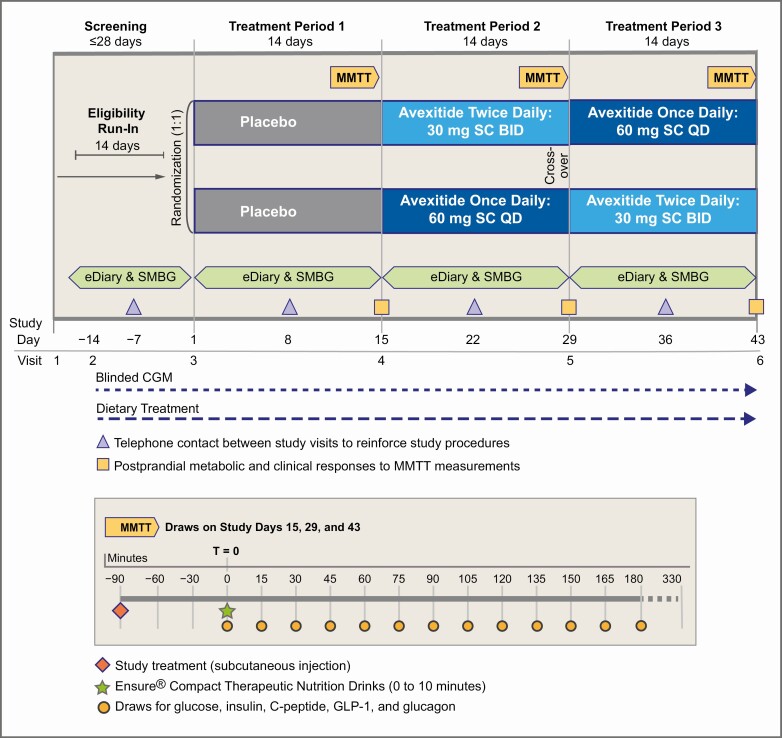
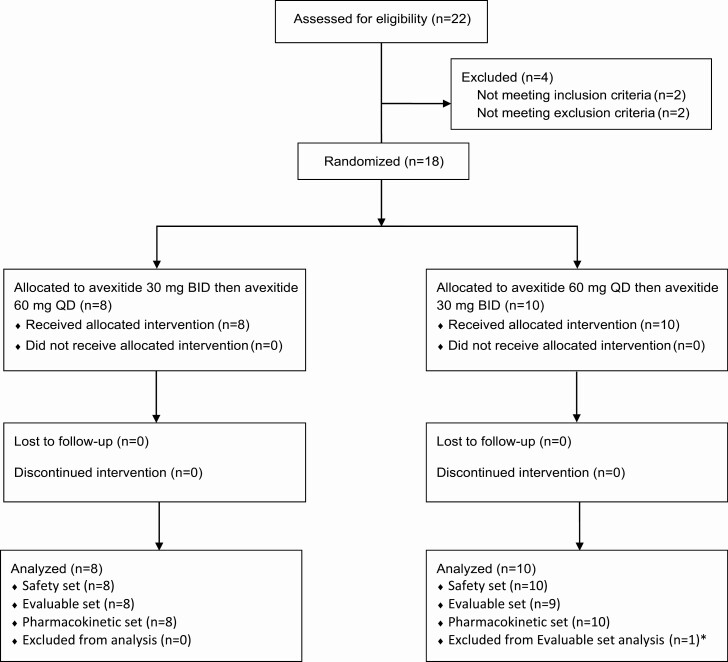
Methods: A multicenter, Phase 2, randomized, placebo-controlled crossover study (PREVENT). Eighteen female patients with PBH were given placebo for 14 days followed by avexitide 30 mg twice daily and 60 mg once daily, each for 14 days in random order. The main outcome measures were glucose nadir and insulin peak during mixed-meal tolerance testing (MMTT) and hypoglycemic events captured by self-monitoring of blood glucose (SMBG), electronic diary, and blinded continuous glucose monitoring (CGM).
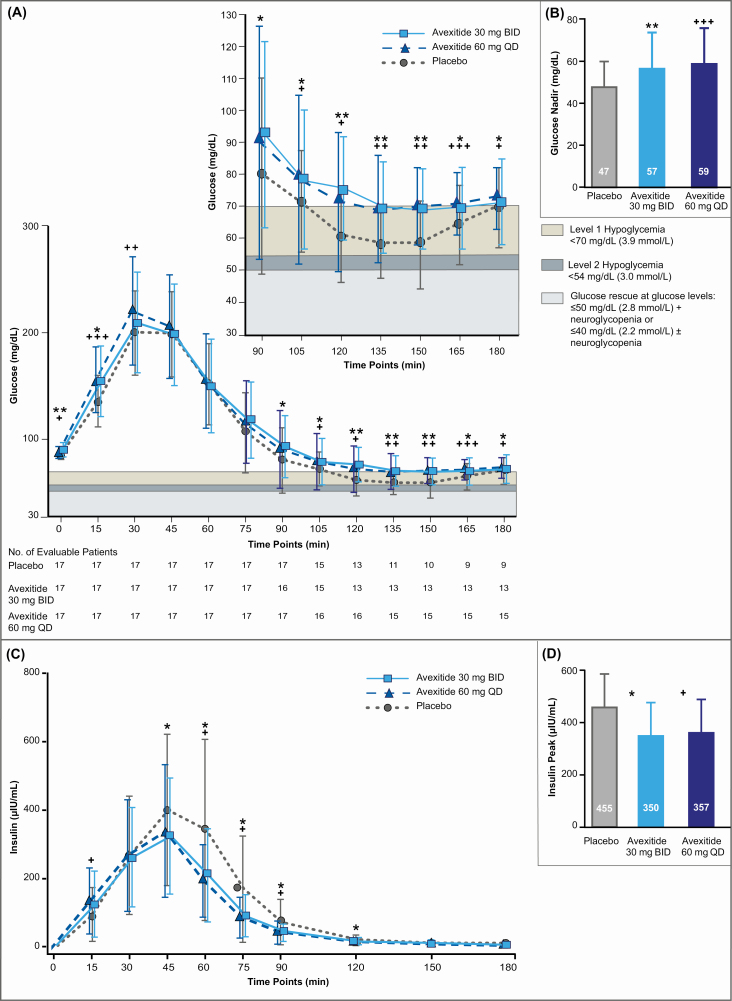
Results: Compared with placebo, avexitide 30 mg twice daily and 60 mg once daily raised the glucose nadir by 21% (P = .001) and 26% (P = .0002) and lowered the insulin peak by 23% (P = .029) and 21% (P = .042), corresponding to 50% and 75% fewer participants requiring rescue during MMTT, respectively. Significant reductions in rates of Levels 1 to 3 hypoglycemia were observed, defined, respectively, as SMBG <70 mg/dL, SMBG <54 mg/dL, and a severe event characterized by altered mental and/or physical function requiring assistance. CGM demonstrated reductions in hypoglycemia without induction of clinically relevant hyperglycemia. Avexitide was well tolerated, with no increase in adverse events.
Conclusion: Avexitide administered for 28 days was well tolerated and resulted in robust and consistent improvements across multiple clinical and metabolic parameters, reinforcing the targeted therapeutic approach and demonstrating durability of effect. Avexitide may represent a first promising treatment for patients with severe PBH.
Trial registration: ClinicalTrials.gov NCT03373435.
Keywords: GLP-1 antagonist; PBH; Postbariatric hypoglycemia; avexitide; exendin (939); hyperinsulinemic hypoglycemia.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
A New Potential Treatment for Postprandial Hypoglycemia Following Bariatric Surgery.J Clin Endocrinol Metab. 2021 Jul 13;106(8):e3264-e3265. doi: 10.1210/clinem/dgab264. J Clin Endocrinol Metab. 2021. PMID: 33880551 No abstract available.
References
-
- Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381(25):2440-2450. - PubMed
-
- Sjöström L, Lindroos AK, Peltonen M, et al. ; Swedish Obese Subjects Study Scientific Group . Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683-2693. - PubMed
-
- Sjöström L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA 2014;311(22):2297-2304. - PubMed
-
- Kwok CS, Pradhan A, Khan MA, et al. Bariatric surgery and its impact on cardiovascular disease and mortality: a systematic review and meta-analysis. Int J Cardiol. 2014;173(1):20-28. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
