

Flow cytometric evaluation of the neutrophil compartment in COVID-19 at hospital presentation: A normal response to an abnormal situation
- PMID: 33617030
- PMCID: PMC10016865
- DOI: 10.1002/JLB.5COVA0820-520RRR
Flow cytometric evaluation of the neutrophil compartment in COVID-19 at hospital presentation: A normal response to an abnormal situation
Abstract
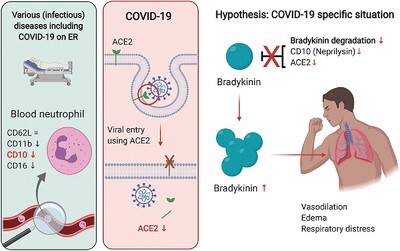
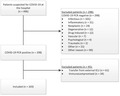
Coronavirus disease 2019 (COVID-19) is a rapidly emerging pandemic disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Critical COVID-19 is thought to be associated with a hyper-inflammatory process that can develop into acute respiratory distress syndrome, a critical disease normally mediated by dysfunctional neutrophils. This study tested the hypothesis whether the neutrophil compartment displays characteristics of hyperinflammation in COVID-19 patients. Therefore, a prospective study was performed on all patients with suspected COVID-19 presenting at the emergency room of a large academic hospital. Blood drawn within 2 d after hospital presentation was analyzed by point-of-care automated flow cytometry and compared with blood samples collected at later time points. COVID-19 patients did not exhibit neutrophilia or eosinopenia. Unexpectedly neutrophil activation markers (CD11b, CD16, CD10, and CD62L) did not differ between COVID-19-positive patients and COVID-19-negative patients diagnosed with other bacterial/viral infections, or between COVID-19 severity groups. In all patients, a decrease was found in the neutrophil maturation markers indicating an inflammation-induced left shift of the neutrophil compartment. In COVID-19 this was associated with disease severity.
Keywords: CD10; SARS‐CoV‐2; activation; flow cytometry; neprilysin; neutrophil.
©2020 Society for Leukocyte Biology.
Figures







References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
