

Does Biceps Tenotomy or Tenodesis Have Better Results After Surgery? A Systematic Review and Meta-analysis
- PMID: 33617158
- PMCID: PMC8208384
- DOI: 10.1097/CORR.0000000000001672
Does Biceps Tenotomy or Tenodesis Have Better Results After Surgery? A Systematic Review and Meta-analysis
Abstract
Background: Although tenotomy and tenodesis are frequently used for long head of the biceps tendon lesions, controversies remain as to which technique is superior regarding pain, functionality, complications, and cosmetic appearance.
Questions/purposes: (1) For long head of biceps tendon lesions, does tenotomy or tenodesis result in greater improvements in VAS score for pain? (2) Which approach has superior results when evaluating function outcome (Constant) scores? (3) Does tenotomy or tenodesis have fewer complications? (4) Does tenotomy or tenodesis result in better cosmesis (Popeye sign)?
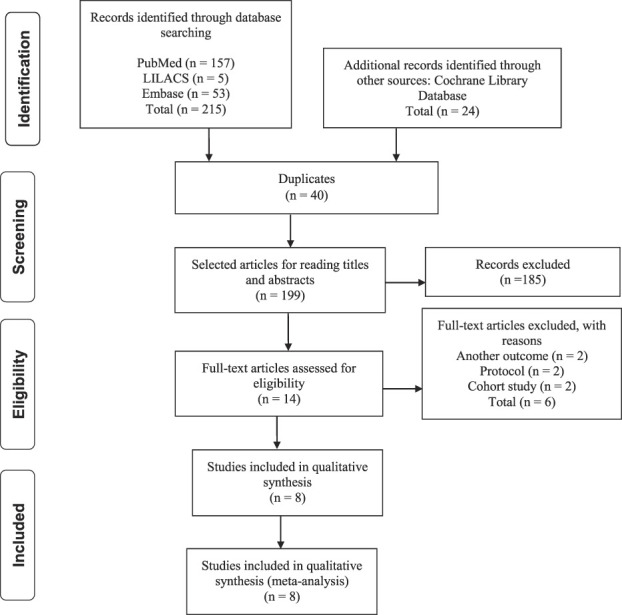
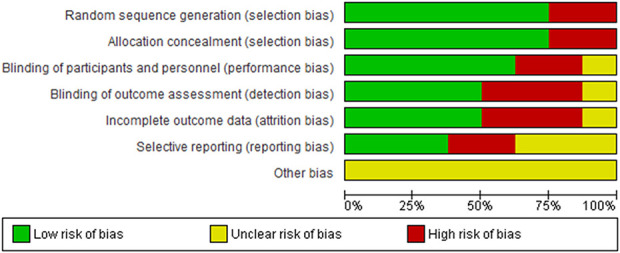
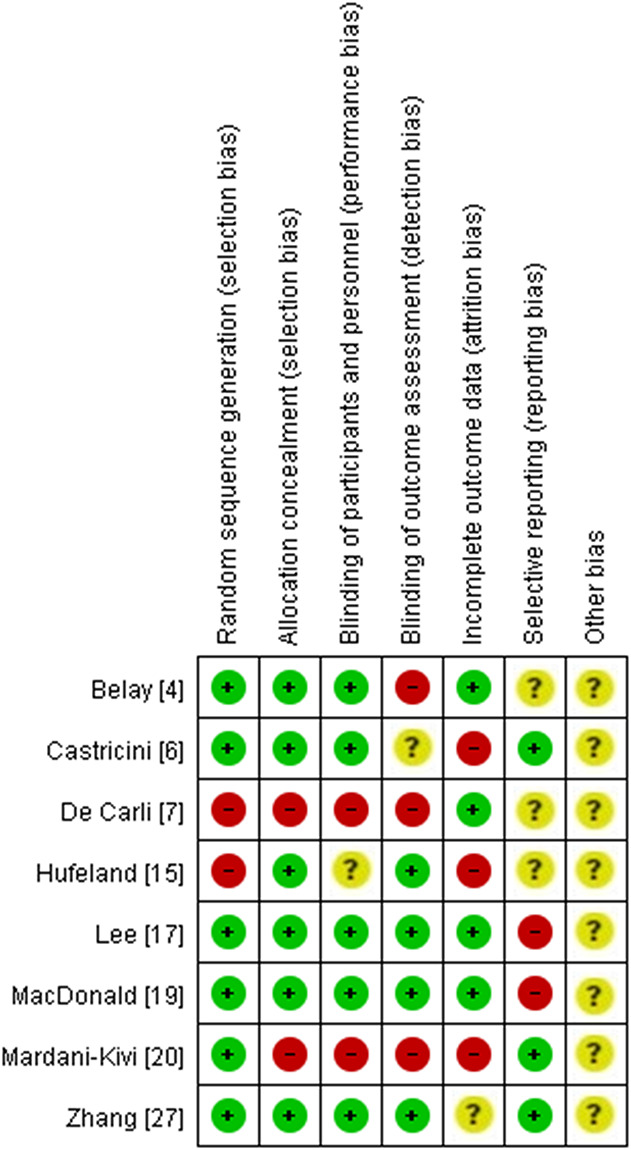
Methods: A systematic review was performed in the Cochrane Library, Embase, PubMed, and Literatura Latino Americana e do Caribe em Ciências da Saúde (LILACS) using the keywords "long head of the biceps tendon," "biceps tenodesis," and "tenotomy." We completed the search in June 2020. The inclusion criteria were randomized controlled trials and quasirandomized controlled trials that investigated tenodesis and tenotomy with no language restriction and evaluation of adult patients who presented with a long head of the biceps tendon lesion, associated with other lesions or not, without previous shoulder surgeries and who had no response to nonoperative treatment. The initial search yielded 239 studies, 40 of which were duplicates. We assessed the titles and abstracts of 199 articles and excluded all studies that were not randomized controlled trials (literature reviews) or that compared different techniques. We assessed the full text of 14 articles and excluded the ones that were protocols and cohort studies. We evaluated the risk of bias using the Cochrane Collaboration tool. We included eight studies in this systematic review and meta-analysis, with a total of 615 participants, 306 of whom were treated with tenotomy and 309 with tenodesis. The median duration of follow-up was 2 years. Overall, the included studies had a low risk of bias. The complications evaluated were adhesive capsulitis, biceps brachii tear, cramps, and a subsequent second surgical procedure. We used a random model in this meta-analysis so that we could generalize the results beyond the included studies. In this study, we only reported differences between the groups if they were both statistically valid and larger than the minimum clinically important difference (MCID).
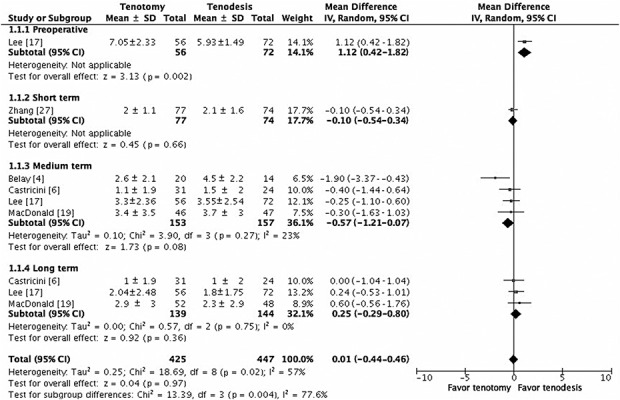
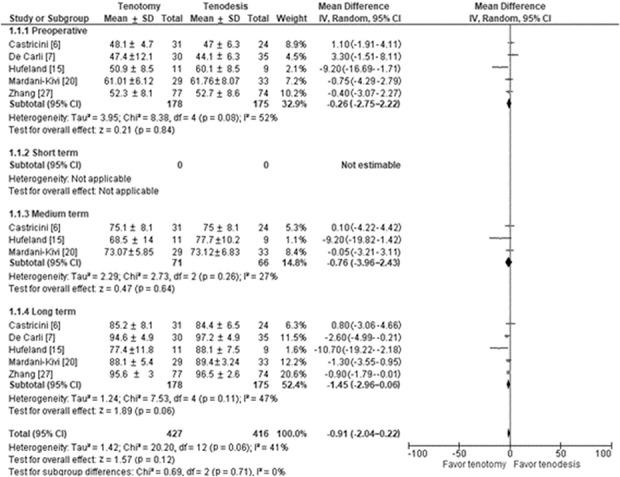
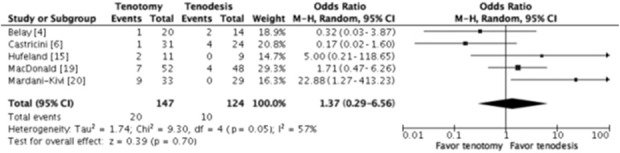
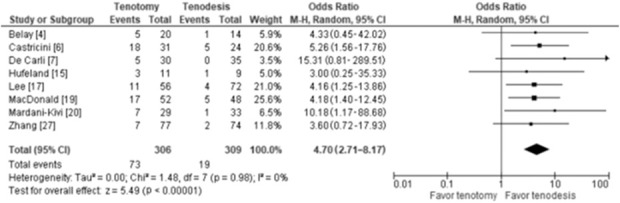
Results: Comparing tenotomy and tenodesis, we observed no difference between the groups regarding pain in the long term (mean difference 0.25 [95% confidence interval -0.29 to 0.80]; p = 0.36). There was no difference in Constant score in the long-term (mean difference -1.45 [95% CI -2.96 to 0.06]; p = 0.06). There were no differences when evaluating for major complications (odds ratio 1.37 [95% CI 0.29 to 6.56]; p = 0.70). There were not enough papers evaluating adhesive capsulitis, cramping, and risk of revision surgery. Popeye sign was more frequent in the tenotomy group than in the tenodesis group (OR 4.70 [95% CI 2.71 to 8.17]; p < 0.001).
Conclusion: This systematic review demonstrated that tenotomy and tenodesis offer satisfactory treatment for long head of the biceps tendon lesions. In terms of pain improvement and Constant score, there was no difference between the techniques, but patients undergoing tenotomy have worse cosmetic results. Therefore, surgeons should choose the technique based on their skills and the patient's expectations of surgery, such as cosmesis and time to recovery. More studies are needed to evaluate complications such as adhesive capsulitis and cramping, as well as to compare duration of surgery and recovery time for each technique.
Level of evidence: Level I, therapeutic study.
Copyright © 2021 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that neither he nor she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Does Biceps Tenotomy or Tenodesis Have Better Results After Surgery? A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2021 Jul 1;479(7):1574-1576. doi: 10.1097/CORR.0000000000001743. Clin Orthop Relat Res. 2021. PMID: 34077395 Free PMC article. No abstract available.
References
-
- Ahmad CS, El Attrache NS. Arthroscopic biceps tenodesis. Orthop Clin North Am. 2003;34:499-506. - PubMed
-
- Anil U, Hurley ET, Kingery MT, Pauzenberger L, Mullett H, Strauss EJ. Surgical treatment for long head of the biceps tendinopathy: a network meta-analysis. J Shoulder Elbow Surg. 2020;29:1289-1295. - PubMed
-
- Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401-406. - PubMed
-
- Belay ES, Wittstein JR, Garrigues GE, et al. Biceps tenotomy has earlier pain relief compared to biceps tenodesis: a randomized prospective study. Knee Surg Sports Traumatol Arthrosc. 2019;27:4032-4037. - PubMed
-
- Boileau P, Baqué F, Valerio L, Ahrens P, Chuinard C, Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007;89:747-757. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
