

Antibiotic Regimens and Associated Outcomes in Children Hospitalized With Staphylococcal Scalded Skin Syndrome
- PMID: 33617441
- PMCID: PMC7929614
- DOI: 10.12788/jhm.3529
Antibiotic Regimens and Associated Outcomes in Children Hospitalized With Staphylococcal Scalded Skin Syndrome
Abstract
Background: Controversy exists regarding the optimal antibiotic regimen for use in hospitalized children with staphylococcal scalded skin syndrome (SSSS). Various regimens may confer toxin suppression and/or additional coverage for methicillin-susceptible Staphylococcus aureus (MSSA) or methicillin-resistant S aureus (MRSA).
Objectives: To describe antibiotic regimens in hospitalized children with SSSS and examine the association between antistaphylococcal antibiotic regimens and patient outcomes.
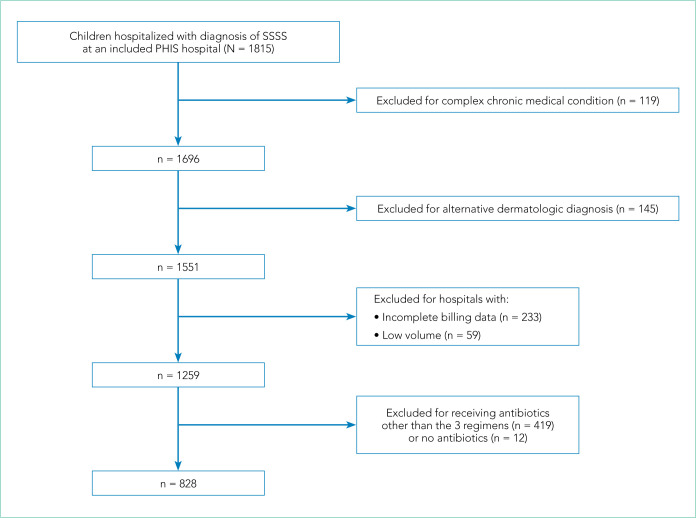
Design/methods: Retrospective cohort study of children hospitalized with SSSS using the Pediatric Health Information System database (2011-2016). Children who received clindamycin monotherapy, clindamycin plus MSSA coverage (eg, nafcillin), or clindamycin plus MRSA coverage (eg, vancomycin) were included. The primary outcome was hospital length of stay (LOS); secondary outcomes were treatment failure and cost. Generalized linear mixed-effects models were used to compare outcomes among antibiotic groups.
Results: Of 1,259 children included, 828 children received the most common antistaphylococcal antibiotic regimens: clindamycin monotherapy (47%), clindamycin plus MSSA coverage (33%), and clindamycin plus MRSA coverage (20%). Children receiving clindamycin plus MRSA coverage had higher illness severity (44%) compared with clindamycin monotherapy (28%) and clindamycin plus MSSA (32%) (P =.001). In adjusted analyses, LOS and treatment failure did not differ among the 3 regimens (P =.42 and P =.26, respectively). Cost was significantly lower for children receiving clindamycin monotherapy and highest in those receiving clindamycin plus MRSA coverage (mean, $4,839 vs $5,348, respectively; P <.001).
Conclusions: In children with SSSS, the addition of MSSA or MRSA coverage to clindamycin monotherapy was associated with increased cost and no incremental difference in clinical outcomes.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
