

Angiotensin-converting enzyme 2 and kidney diseases in the era of coronavirus disease 2019
- PMID: 33617712
- PMCID: PMC7969072
- DOI: 10.3904/kjim.2020.355
Angiotensin-converting enzyme 2 and kidney diseases in the era of coronavirus disease 2019
Abstract
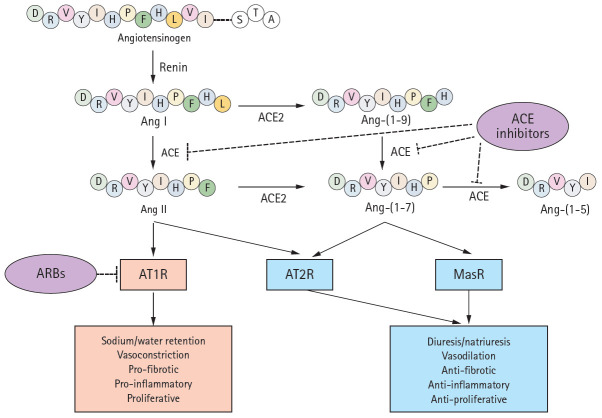
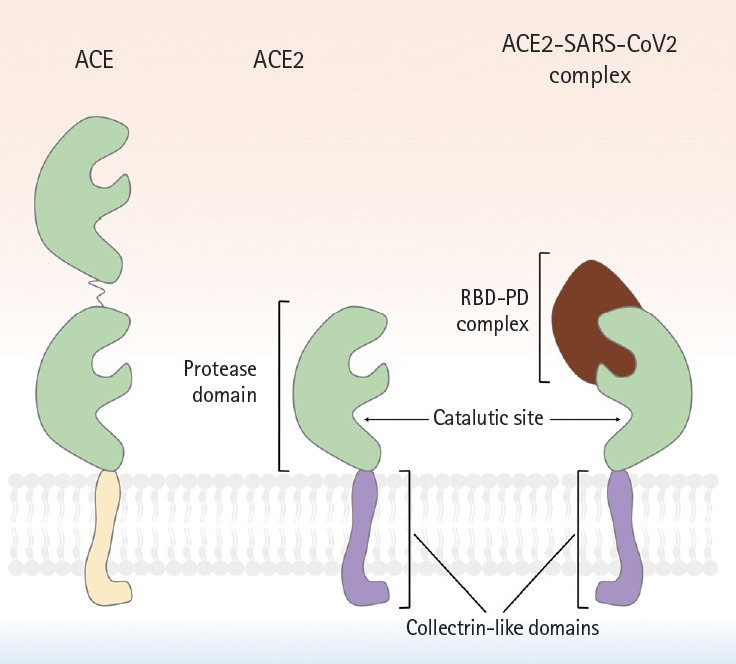
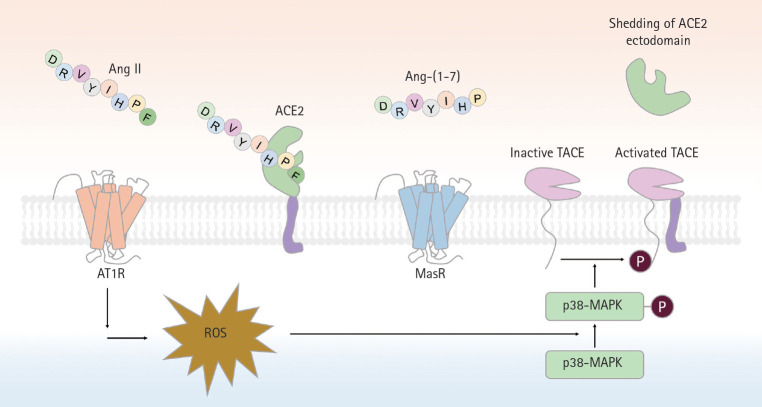
In the decades since the discovery of angiotensin-converting enzyme 2 (ACE2), its protective role in terms of antagonizing activation of the classical renin-angiotensin system (RAS) axis has been recognized in clinical and experimental studies on kidney and cardiovascular diseases. The effects of ACE inhibitor/angiotensin type 1 receptor blockers (ACEi/ARBs) on ACE2-angiotensin-(1-7) (Ang- (1-7))-Mas receptor (MasR) axis activation has encouraged the use of such blockers in patients with kidney and cardiovascular diseases, until the emergence of coronavirus disease 2019 (COVID-19). The previously unchallenged functions of the ACE2-Ang-(1-7)-MasR axis and ACEi/ARBs are being re-evaluated in the era of COVID-19; the hypothesis is that ACEi/ARBs may increase the risk of severe acute respiratory syndrome coronavirus 2 infection by upregulating the human ACE2 receptor expression level. In this review, we examine ACE2 molecular structure, function (as an enzyme of the RAS), and distribution. We explore the roles played by ACE2 in kidney, cardiovascular, and pulmonary diseases, highlighting studies that defined the benefits imparted when ACEi/ARBs activated the local ACE2- Ang-(1-7)-MasR axis. Finally, the question of whether ACEi/ARBs therapies should be stopped in COVID-19-infected patients will be reviewed by reference to the available evidence.
Keywords: Angiotensin converting enzyme 2; COVID-19; Cardiovascular diseases; Kidney diseases; Severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Angiotensin-Converting-Enzyme 2 and Renin-Angiotensin System Inhibitors in COVID-19: An Update.High Blood Press Cardiovasc Prev. 2021 Mar;28(2):129-139. doi: 10.1007/s40292-021-00439-9. Epub 2021 Feb 26. High Blood Press Cardiovasc Prev. 2021. PMID: 33635533 Free PMC article. Review.
-
Expression of the SARS-CoV-2 receptorACE2 in human heart is associated with uncontrolled diabetes, obesity, and activation of the renin angiotensin system.Cardiovasc Diabetol. 2021 Apr 27;20(1):90. doi: 10.1186/s12933-021-01275-w. Cardiovasc Diabetol. 2021. PMID: 33906662 Free PMC article.
-
ACE2, the kidney and the emergence of COVID-19 two decades after ACE2 discovery.Clin Sci (Lond). 2020 Nov 13;134(21):2791-2805. doi: 10.1042/CS20200484. Clin Sci (Lond). 2020. PMID: 33135725 Review.
-
ACE2: from protection of liver disease to propagation of COVID-19.Clin Sci (Lond). 2020 Dec 11;134(23):3137-3158. doi: 10.1042/CS20201268. Clin Sci (Lond). 2020. PMID: 33284956 Review.
-
Foe and friend in the COVID-19-associated acute kidney injury: an insight on intrarenal renin-angiotensin system.Acta Biochim Biophys Sin (Shanghai). 2022 Jan 25;54(1):1-11. doi: 10.3724/abbs.2021002. Acta Biochim Biophys Sin (Shanghai). 2022. PMID: 35130610 Free PMC article. Review.
Cited by
-
Albumin: A Review of Market Trends, Purification Methods, and Biomedical Innovations.Curr Issues Mol Biol. 2025 Apr 26;47(5):303. doi: 10.3390/cimb47050303. Curr Issues Mol Biol. 2025. PMID: 40699702 Free PMC article. Review.
-
Urinary Angiotensinogen and Progression of Chronic Kidney Disease: Results from KNOW-CKD Study.Biomolecules. 2022 Sep 10;12(9):1280. doi: 10.3390/biom12091280. Biomolecules. 2022. PMID: 36139118 Free PMC article.
-
Review: Roles of human serum albumin in prediction, diagnoses and treatment of COVID-19.Int J Biol Macromol. 2021 Dec 15;193(Pt A):948-955. doi: 10.1016/j.ijbiomac.2021.10.095. Epub 2021 Oct 18. Int J Biol Macromol. 2021. PMID: 34673106 Free PMC article. Review.
-
Studying the Roles of the Renin-Angiotensin System in Accelerating the Disease of High-Fat-Diet-Induced Diabetic Nephropathy in a db/db and ACE2 Double-Gene-Knockout Mouse Model.Int J Mol Sci. 2023 Dec 26;25(1):329. doi: 10.3390/ijms25010329. Int J Mol Sci. 2023. PMID: 38203500 Free PMC article.
References
-
- Donoghue M, Hsieh F, Baronas E, et al. A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1-9. Circ Res. 2000;87:E1–E9. - PubMed
-
- Tipnis SR, Hooper NM, Hyde R, Karran E, Christie G, Turner AJ. A human homolog of angiotensin-converting enzyme. Cloning and functional expression as a captopril-insensitive carboxypeptidase. J Biol Chem. 2000;275:33238–33243. - PubMed
-
- Higuchi S, Ohtsu H, Suzuki H, Shirai H, Frank GD, Eguchi S. Angiotensin II signal transduction through the AT1 receptor: novel insights into mechanisms and pathophysiology. Clin Sci (Lond) 2007;112:417–428. - PubMed
-
- Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001 Sep;345:861–869. - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851–860. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous