

Communication and Virtual Visiting for Families of Patients in Intensive Care during the COVID-19 Pandemic: A UK National Survey
- PMID: 33617747
- PMCID: PMC8522289
- DOI: 10.1513/AnnalsATS.202012-1500OC
Communication and Virtual Visiting for Families of Patients in Intensive Care during the COVID-19 Pandemic: A UK National Survey
Abstract
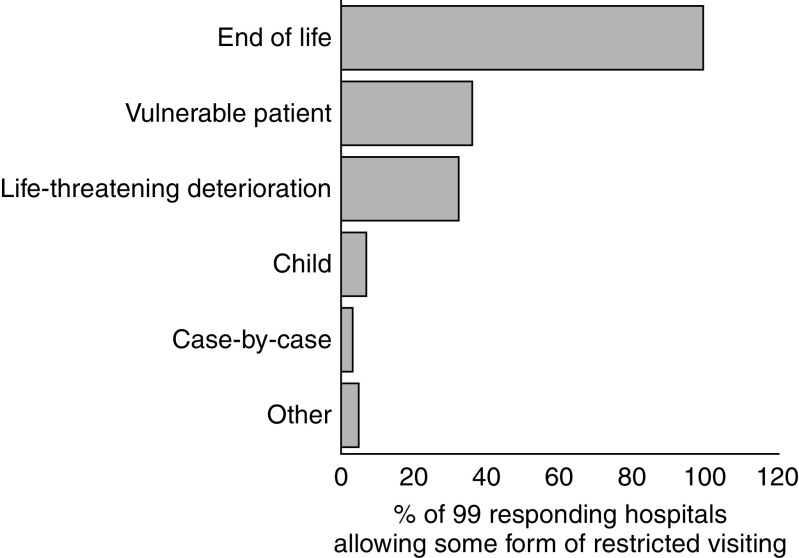
Rationale: Restriction or prohibition of family visiting intensive care units (ICUs) during the coronavirus disease (COVID-19) pandemic poses substantial barriers to communication and family- and patient-centered care. Objectives: To understand how communication among families, patients, and the ICU team was enabled during the pandemic. The secondary objectives were to understand strategies used to facilitate virtual visiting and associated benefits and barriers. Methods: A multicenter, cross-sectional, and self-administered electronic survey was sent (June 2020) to all 217 UK hospitals with at least one ICU. Results: The survey response rate was 54%; 117 of 217 hospitals (182 ICUs) responded. All hospitals imposed visiting restrictions, with visits not permitted under any circumstance in 16% of hospitals (28 ICUs); 63% (112 ICUs) of hospitals permitted family presence at the end of life. The responsibility for communicating with families shifted with decreased bedside nurse involvement. A dedicated ICU family-liaison team was established in 50% (106 ICUs) of hospitals. All but three hospitals instituted virtual visiting, although there was substantial heterogeneity in the videoconferencing platform used. Unconscious or sedated ICU patients were deemed ineligible for virtual visits in 23% of ICUs. Patients at the end of life were deemed ineligible for virtual visits in 7% of ICUs. Commonly reported benefits of virtual visiting were reducing patient psychological distress (78%), improving staff morale (68%), and reorientation of patients with delirium (47%). Common barriers to virtual visiting were related to insufficient staff time, rapid implementation of videoconferencing technology, and challenges associated with family members' ability to use videoconferencing technology or access a device. Conclusions: Virtual visiting and dedicated communication teams were common COVID-19 pandemic innovations addressing the restrictions to family ICU visiting, and they resulted in valuable benefits in terms of patient recovery and staff morale. Enhancing access and developing a more consistent approach to family virtual ICU visits could improve the quality of care, both during and outside of pandemic conditions.
Keywords: COVID-19; communication; family; intensive care; visiting.
Figures

References
-
- National Health Service England. London, UK: National Health Service; 2020. http://www.yhscn.nhs.uk/media/PDFs/mhdn/Dementia/Covid%2019/C0030_Visito...
-
- National Health Service England. London, UK: National Health Service; 2020. https://www.england.nhs.uk/coronavirus/publication/visitor-guidance/
-
- Wynia MK. Ethics and public health emergencies: restrictions on liberty. Am J Bioeth. 2007;7:1–5. - PubMed
-
- Executive Office of the President. Respecting the rights of hospital patients to receive visitors and to designate surrogate decision makers for medical emergencies. Federal Register. 2010;75:20511–20512.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
