

Impact and Determinants of High-Sensitivity Cardiac Troponin-T Concentration in Patients With COVID-19 Admitted to Critical Care
- PMID: 33617816
- PMCID: PMC7895690
- DOI: 10.1016/j.amjcard.2021.01.037
Impact and Determinants of High-Sensitivity Cardiac Troponin-T Concentration in Patients With COVID-19 Admitted to Critical Care
Abstract
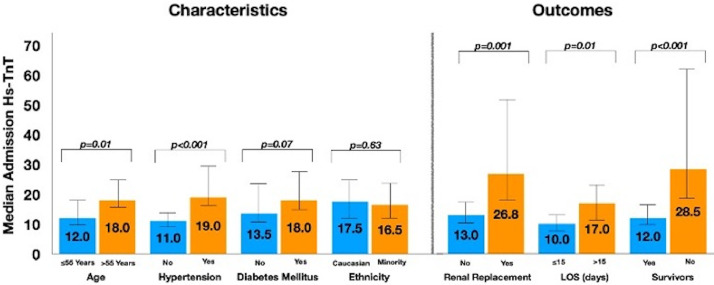
Cardiac Troponin (hs-TnT) elevation has been reported in unselected patients hospitalized with COVID-19 however the mechanism and relationship with mortality remain unclear. Consecutive patients admitted to a high-volume intensive care unit (ICU) in London with severe COVID-19 pneumonitis were included if hs-TnT concentration at admission was known. Kaplan-Meier survival analysis performed, with cohorts classified a priori by multiples of the upper limit of normal (ULN). 277 patients were admitted during a 7-week period in 2020; 176 were included (90% received invasive ventilation). hs-TnT at admission was 16.5 (9.0 to 49.3) ng/L, 56% had concentrations >ULN. 56 patients (31.8%) died during the index admission. Admission hs-TnT level was lower in survivors (12.0 (8.0-27.8) vs 28.5 (14.0 to 81.0) ng/L, p = 0.001). Univariate predictors of mortality were age, APACHE-II Score and admission hs-TnT (HR 1.73, p = 0.007). By multivariate regression, only age (HR 1.33, CI: 1.16.to 1.51, p < 0.01) and admission hs-TnT (HR 1.94, CI: 1.22 to 3.10, p = 0.006) remained predictive. Survival was significantly lower when admission hs-TnT was >ULN (log-rank p-value<0.001). Peak hs-TnT was higher in those who died but was not predictive of death after adjustment for other factors. In conclusion, in critically ill patients with COVID-19 pneumonitis, the hs-TnT level at admission is a powerful independent predictor of the likelihood of surviving to discharge from ICU. In most cases, hs-TnT elevation does not represent major myocardial injury but acts as a sensitive integrated biomarker of global stress. Whether stratification based on admission Troponin level could be used to guide prognostication and management warrants further evaluation.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests The authors declare that they have no known competing financial interests or personal relations that could have appeared to influence the work reported in this study.
Figures




References
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk DA, Kim EJ, Kozel ZM, Marrast LM, Mogavero JN, Osorio GA, Qiu M, Zanos TP. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA. 2020;323:2052–2059. - PMC - PubMed
-
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. - PMC - PubMed
-
- Lala A, Johnson KW, Januzzi JL, Russak AJ, Paranjpe I, Richter F, Zhao S, Somani S, Van Vleck T, Vaid A, Chaudhry F, De Freitas JK, Fayad ZA, Pinney SP, Levin M, Charney A, Bagiella E, Narula J, Glicksberg BS, Nadkarni G, Mancini DM, Fuster V. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol. 2020;76:533–546. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
