

Economic burden of recurrent Clostridioides difficile infection in adults admitted to Spanish hospitals. A multicentre retrospective observational study
- PMID: 33618513
- PMCID: PMC8019457
- DOI: 10.37201/req/135.2020
Economic burden of recurrent Clostridioides difficile infection in adults admitted to Spanish hospitals. A multicentre retrospective observational study
Abstract
Objective: Clostridioides difficile infection (CDI) is associated with increased hospital stays and mortality and a high likelihood of rehospitalization, leading to increased health resource use and costs. The objective was to estimate the economic burden of recurrent CDI (rCDI).
Methods: Observational, retrospective study carried out in six hospitals. Adults aged ≥18 years with ≥1 confirmed diagnosis (primary or secondary) of rCDI between January 2010 and May 2018 were included. rCDI-related resource use included days of hospital stay (emergency room, ward, isolation and ICU), tests and treatments. For patients with primary diagnosis of rCDI, the complete hospital stay was attributed to rCDI. When diagnosis of rCDI was secondary, hospital stay attributed to rCDI was estimated using 1:1 propensity score matching as the difference in hospital stay compared to controls. Controls were hospitalizations without CDI recorded in the Spanish National Hospital Discharge Database. The cost was calculated by multiplying the natural resource units by the unit cost. Costs (euros) were updated to 2019.
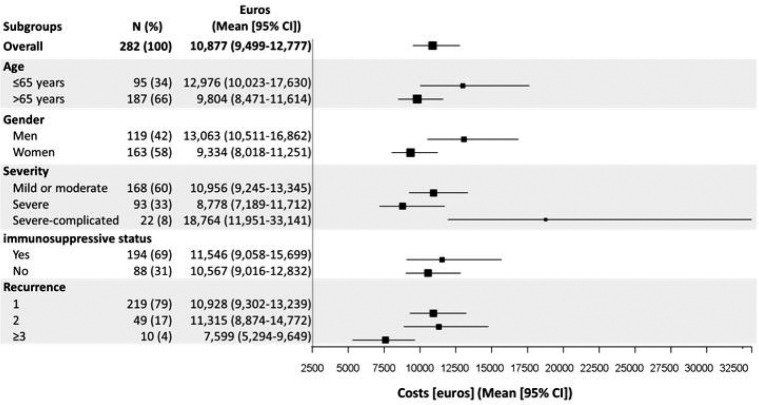
Results: We included 282 rCDI episodes (188 as primary diagnosis): 66.31% of patients were aged ≥65 years and 57.80% were female. The mean hospital stay (SD) was 17.18 (23.27) days: 86.17% of rCDI episodes were isolated for a mean (SD) of 10.30 (9.97) days. The total mean cost (95%-CI) per episode was €10,877 (9,499-12,777), of which the hospital stay accounted for 92.56.
Conclusions: There is high cost and resource use associated with rCDI, highlighting the importance of preventing rCDI to the Spanish National Health System.
Introducción: La infección por Clostridioides difficile (ICD) está asociada a un aumento de la estancia hospitalaria y de la mortalidad y a una alta probabilidad de reingreso, lo que conlleva un aumento de uso de recursos sanitarios y por tanto un incremento de costes. El objetivo del estudio fue estimar la carga económica de la ICD recurrente (ICDr).
Material y métodos: Estudio observacional, retrospectivo y multicéntrico. Se incluyeron pacientes adultos (≥18 años), que tuvieran registrado al menos un episodio diagnóstico confirmado (primario o secundario) de ICDr durante enero 2010 y mayo 2018. El uso de recursos relacionado con la ICDr incluyó la estancia hospitalaria (urgencias previas, planta, aislamiento y UCI), así como pruebas y tratamientos. Para episodios que ingresaron por ICDr (diagnóstico principal) se consideró la estancia completa registrada. Cuando la ICDr se registró como diagnóstico secundario se estimó la estancia hospitalaria debida a ICDr mediante emparejamiento (1:1) utilizando la técnica “propensity score”. Se consideraron como controles (episodios sin ICD) las hospitalizaciones registradas en Conjunto Mínimo Básico de las Altas Hospitalarias. El coste total se calculó multiplicando las unidades naturales de los recursos por el coste unitario correspondiente. Todos los costes fueron actualizados a euros de 2019.
Resultados: Se incluyeron 282 episodios ICDr (188 como diagnóstico principal): 66,31% de los pacientes tenían más de 65 años y 57,80% eran mujeres. La estancia media (DE) hospitalaria fue de 17,18 (23,27) días. Un 86,17% de los episodios fueron aislados debido a ICDr con una media (DE) de 10,30 (9,97) días. El coste medio (IC-95%) total por episodio fue de 10.877€ (9.499-12.777), siendo la duración de la estancia hospitalaria el 92,56% del coste total.
Conclusiones: Tanto el uso de recursos como el coste debido a la ICDr tienen un alto impacto para el sistema nacional de salud lo que pone de relieve la importancia de prevenir las ICDr.
Keywords: Clostridioides difficile; ost analysis; recurrence.
©The Author 2021. Published by Sociedad Española de Quimioterapia. This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)(https://creativecommons.org/licenses/by-nc/4.0/).
Conflict of interest statement
EB, has participated in clinical trials and advisory boards sponsored by MSD, Pfizer and Astellas. JC received fees as a speaker in conferences and advisory board meetings from Astellas and MSD. MJR-H received fees as a speaker and participant in advisory board meetings from Astellas and MSD. MS has lectured at meetings organized by pharmaceutical companies (MSD, Janssen, Pfizer and Gilead) or participated in some medical advice. He has not received direct grants or scholarships. JPH has received fees as a speaker and participant in advisory board meetings from Pfizer, MSD, Menarini and Zambon and a research grant from MSD. JAI reported no conflicts of interest. EO is an employee of Merck & Co. VL is an employee of Merck Sharp & Dohme. SM was an employee of Merck Sharp & Dohme. MC and EU are employees of Oblikue Consulting. EL declares he has been a speaker in a symposium organized by MSD.
Figures


Similar articles
-
Healthcare burden of recurrent Clostridioides difficile infection in Japan: A retrospective database study.J Infect Chemother. 2018 Nov;24(11):892-901. doi: 10.1016/j.jiac.2018.07.020. Epub 2018 Sep 3. J Infect Chemother. 2018. PMID: 30190105
-
Predictors and burden of hospital readmission with recurrent Clostridioides difficile infection: a French nation-wide inception cohort study.Eur J Clin Microbiol Infect Dis. 2019 Jul;38(7):1297-1305. doi: 10.1007/s10096-019-03552-9. Epub 2019 Apr 2. Eur J Clin Microbiol Infect Dis. 2019. PMID: 30941532
-
Healthcare resource utilization and direct medical costs associated with index and recurrent Clostridioides difficile infection: a real-world data analysis.J Med Econ. 2020 Jun;23(6):603-609. doi: 10.1080/13696998.2020.1724117. Epub 2020 Feb 13. J Med Econ. 2020. PMID: 31999199
-
Economic Impact of Recurrent Clostridioides difficile Infection in the USA: A Systematic Literature Review and Cost Synthesis.Adv Ther. 2023 Jul;40(7):3104-3134. doi: 10.1007/s12325-023-02498-x. Epub 2023 May 21. Adv Ther. 2023. PMID: 37210680 Free PMC article.
-
Trends in and Risk Factors for Recurrent Clostridioides difficile Infection, New Haven County, Connecticut, USA, 2015-2020.Emerg Infect Dis. 2023 May;29(5):877-87. doi: 10.3201/eid2905.221294. Emerg Infect Dis. 2023. PMID: 37081745 Free PMC article. Review.
Cited by
-
Economic Burden of Clostridioides difficile Infection in European Countries.Adv Exp Med Biol. 2024;1435:1-12. doi: 10.1007/978-3-031-42108-2_1. Adv Exp Med Biol. 2024. PMID: 38175468
-
Evaluating Bezlotoxumab-Fidaxomicin Combination Therapy in Clostridioides Infection: A Single-Center Retrospective Study from Aichi Prefecture, Japan.Antibiotics (Basel). 2025 Feb 24;14(3):228. doi: 10.3390/antibiotics14030228. Antibiotics (Basel). 2025. PMID: 40149040 Free PMC article.
-
Retrospective Analysis of Clostridioides difficile Infection Rates and Outcomes in Hospitalized Patients during the COVID-19 Pandemic: A Unicenter Study in Reus, Spain.J Clin Med. 2024 May 9;13(10):2799. doi: 10.3390/jcm13102799. J Clin Med. 2024. PMID: 38792341 Free PMC article.
-
Detection of Beta-Lactam-Resistant Escherichia coli and Toxigenic Clostridioides difficile Strains in Wild Boars Foraging in an Anthropization Gradient.Animals (Basel). 2021 May 28;11(6):1585. doi: 10.3390/ani11061585. Animals (Basel). 2021. PMID: 34071332 Free PMC article.
-
Treatment of Clostridioides difficile infection: from guidelines to clinical practice.Rev Esp Quimioter. 2022 Oct;35 Suppl 3(Suppl 3):97-101. doi: 10.37201/req/s03.21.2022. Epub 2022 Oct 24. Rev Esp Quimioter. 2022. PMID: 36285868 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
