

Systematic evaluation of nine monogenic autoinflammatory diseases reveals common and disease-specific correlations with allergy-associated features
- PMID: 33619160
- PMCID: PMC8380268
- DOI: 10.1136/annrheumdis-2020-219137
Systematic evaluation of nine monogenic autoinflammatory diseases reveals common and disease-specific correlations with allergy-associated features
Abstract
Background: Monogenic autoinflammatory diseases (AID) are caused by mutations in innate immune genes. The effects of these mutations on allergic inflammation are unknown.
Objectives: We investigated allergic, immunological and clinical phenotypes in FMF (familial Mediterranean fever), CAPS (cryopyrin-associated periodic syndrome), TRAPS (tumour necrosis factor receptor-associated periodic syndrome), HIDS (hyper-IgD syndrome), PAPA (pyogenic arthritis, pyoderma gangrenosum and acne), DADA2 (deficiency of adenosine deaminase 2), HA20 (haploinsufficiency of A20), CANDLE (chronic atypical neutrophilic dermatosis, lipodystrophy, elevated temperature) and SAVI (STING-associated vasculopathy of infancy).
Methods: In this cross-sectional study, clinical data were assessed in 425 patients with AID using questionnaires and chart reviews. Comparator data were obtained from public databases. Peripheral blood mononuclear cells obtained from 55 patients were stimulated and CD4+ cytokine production assessed.
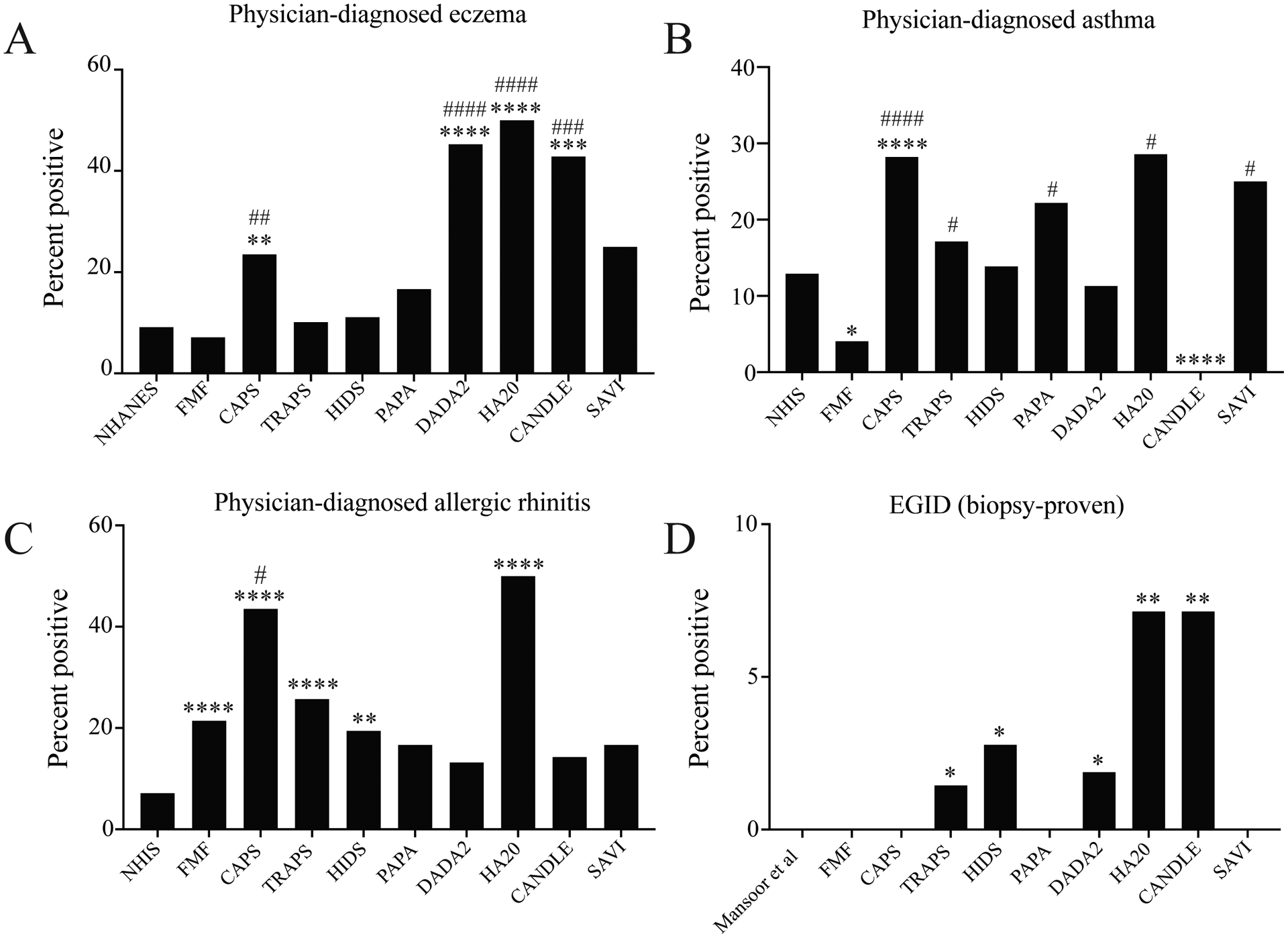
Results: Clinical laboratory features of Type 2 immunity were elevated in CAPS but reduced in most AID, particularly DADA2. Physician-diagnosed allergic diseases were prevalent in multiple AID, including CAPS and DADA2. T helper 2 (Th2) cells were expanded in CAPS, TRAPS and HIDS; Th9 cells were expanded in HA20.
Conclusions: CAPS is characterised by an enhanced Type 2 signature, whereas FMF and CANDLE are associated with reduced Type 2 responses. DADA2 is associated with reduced Type 2 responses but a high rate of physician-diagnosed allergy. Therefore, NLRP3-driven autoinflammation may promote Type 2 immunity, whereas AID like DADA2 may manifest clinical phenotypes that masquerade as allergic disorders. Further investigations are needed to determine the contribution of autoinflammation to allergic clinical and immunological phenotypes, to improve the treatment of patients with AID.
Keywords: T-lymphocyte subsets; cryopyrin-associated periodic syndromes; epidemiology; familial mediterranean fever; inflammation.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Investigators N. Demographics, Laboratory, and Questionnaire Data. National Health and Nutrition Examination Survey. National Center for Health Statistics, 2005–2006.
-
- Investigators N. Tables of Summary Health Statistics for public use. National Health Interview Survey. National Center for Health Statistics, 2015–2018.
-
- Gupta RS, Kim JS, Springston EE, et al. Development of the Chicago Food Allergy Research Surveys: assessing knowledge, attitudes, and beliefs of parents, physicians, and the general public. BMC Health Serv Res 2009;9:142. doi: 10.1186/1472-6963-9-142 [published Online First: 2009/08/12] - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
