

Predictive values of multiple non-invasive markers for myocardial fibrosis in hypertrophic cardiomyopathy patients with preserved ejection fraction
- PMID: 33619345
- PMCID: PMC7900233
- DOI: 10.1038/s41598-021-83678-z
Predictive values of multiple non-invasive markers for myocardial fibrosis in hypertrophic cardiomyopathy patients with preserved ejection fraction
Abstract
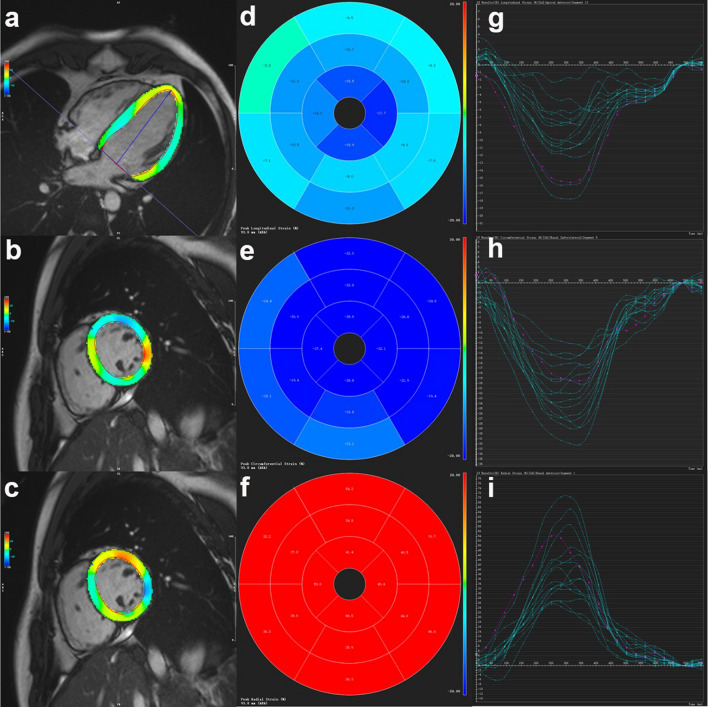
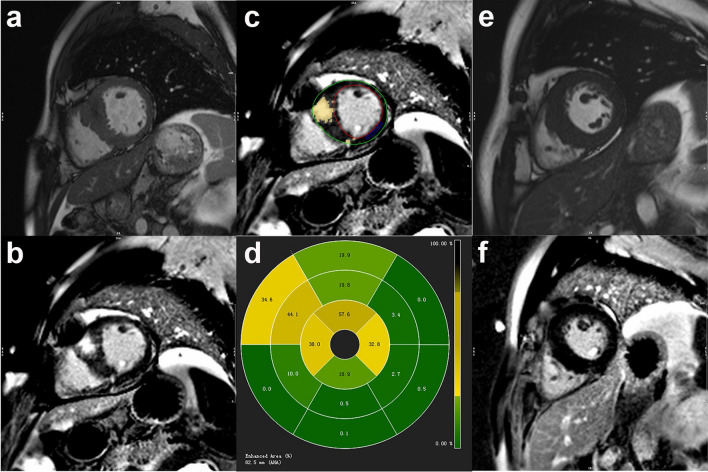
Myocardial fibrosis assessed by late gadolinium enhancement (LGE) on cardiovascular magnetic resonance (CMR) is associated with cardiovascular outcomes in hypertrophic cardiomyopathy (HCM) patients, but little is known about the utility of non-invasive markers for detecting LGE. This study aims to explore the association between cardiac-specific biomarkers, CMR myocardial strain, left ventricular (LV) hypertrophy and LGE in HCM patients with preserved ejection fraction (EF) and investigate the predictive values of these indexes for LGE. We recruited 33 healthy volunteers and 86 HCM patients with preserved EF to undergo contrast-enhanced CMR examinations. In total, 48 of 86 HCM patients had the presence of LGE. The LGE-positive patients had significant higher serum high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro b-type natriuretic peptide (Nt-proBNP) levels and lower global longitudinal (GLS) and circumferential (GCS) strains than the LGE-negative group. The LGE% was independently associated with the Nt-proBNP levels, GCS, LV end-diastolic maximum wall thickness (MWT) and beta-blocker treatment. In the receiver operating characteristic curve analysis, the combined parameters of Nt-proBNP ≥ 108.00 pg/mL and MWT ≥ 17.30 mm had good diagnostic performance for LGE, with a specificity of 81.25% and sensitivity of 70.00%. These data indicate that serum Nt-proBNP is a potential biomarker associated with LGE% and, combined with MWT, were useful for identifying myocardial fibrosis in HCM patients with preserved EF. Additionally, LV GCS may be a more sensitive indicator for reflecting the presence of myocardial fibrosis than GLS.
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Predictive Values of N-Terminal Pro-B-Type Natriuretic Peptide and Cardiac Troponin I for Myocardial Fibrosis in Hypertrophic Obstructive Cardiomyopathy.PLoS One. 2016 Jan 14;11(1):e0146572. doi: 10.1371/journal.pone.0146572. eCollection 2016. PLoS One. 2016. PMID: 26765106 Free PMC article.
-
CMR feature tracking strain patterns and their association with circulating cardiac biomarkers in patients with hypertrophic cardiomyopathy.Clin Res Cardiol. 2021 Nov;110(11):1757-1769. doi: 10.1007/s00392-021-01848-5. Epub 2021 Mar 29. Clin Res Cardiol. 2021. PMID: 33779809 Free PMC article.
-
Evaluation the relationship between myocardial fibrosis and left ventricular torsion measured by cardiac magnetic resonance feature-tracking in hypertrophic cardiomyopathy patients with preserved ejection fraction.Int J Cardiovasc Imaging. 2024 Apr;40(4):921-930. doi: 10.1007/s10554-024-03061-7. Epub 2024 Mar 7. Int J Cardiovasc Imaging. 2024. PMID: 38448705
-
The current and emerging role of cardiovascular magnetic resonance imaging in hypertrophic cardiomyopathy.J Cardiovasc Transl Res. 2009 Dec;2(4):415-25. doi: 10.1007/s12265-009-9136-3. Epub 2009 Nov 7. J Cardiovasc Transl Res. 2009. PMID: 20560000 Review.
-
Contemporary review on pediatric hypertrophic cardiomyopathy: insights into detection and management.Front Cardiovasc Med. 2024 Jan 4;10:1277041. doi: 10.3389/fcvm.2023.1277041. eCollection 2023. Front Cardiovasc Med. 2024. PMID: 38250029 Free PMC article. Review.
Cited by
-
Association between cardiac dysfunction and late gadolinium enhancement confined to the LV intramural region in patients with hypertrophic cardiomyopathy.Ann Med. 2025 Dec;57(1):2533425. doi: 10.1080/07853890.2025.2533425. Epub 2025 Jul 23. Ann Med. 2025. PMID: 40698385 Free PMC article.
-
Impaired hemodynamic forces assessed by routine CMR and its determinants in different duration T2DM patients with normal LV function and myocardial strain.Front Cardiovasc Med. 2025 Jan 31;12:1460094. doi: 10.3389/fcvm.2025.1460094. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 39957999 Free PMC article.
-
Identification of Functional Genetic Determinants of Cardiac Troponin T and I in a Multiethnic Population and Causal Associations With Atrial Fibrillation.Circ Genom Precis Med. 2021 Dec;14(6):e003460. doi: 10.1161/CIRCGEN.121.003460. Epub 2021 Nov 4. Circ Genom Precis Med. 2021. PMID: 34732054 Free PMC article.
-
Imaging in Hypertrophic Cardiomyopathy: Beyond Risk Stratification.Heart Fail Clin. 2023 Oct;19(4):419-428. doi: 10.1016/j.hfc.2023.03.004. Epub 2023 Apr 29. Heart Fail Clin. 2023. PMID: 37714584 Free PMC article. Review.
-
Association of fibrotic markers with diastolic function after STEMI.Sci Rep. 2024 Aug 18;14(1):19122. doi: 10.1038/s41598-024-69926-y. Sci Rep. 2024. PMID: 39155333 Free PMC article.
References
-
- Elliott PM, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) Eur. Heart J. 2014;35:2733–2779. doi: 10.1093/eurheartj/ehu199. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
