

This is a preprint.
Mapping of SARS-CoV-2 Brain Invasion and Histopathology in COVID-19 Disease
- PMID: 33619496
- PMCID: PMC7899461
- DOI: 10.1101/2021.02.15.21251511
Mapping of SARS-CoV-2 Brain Invasion and Histopathology in COVID-19 Disease
Abstract
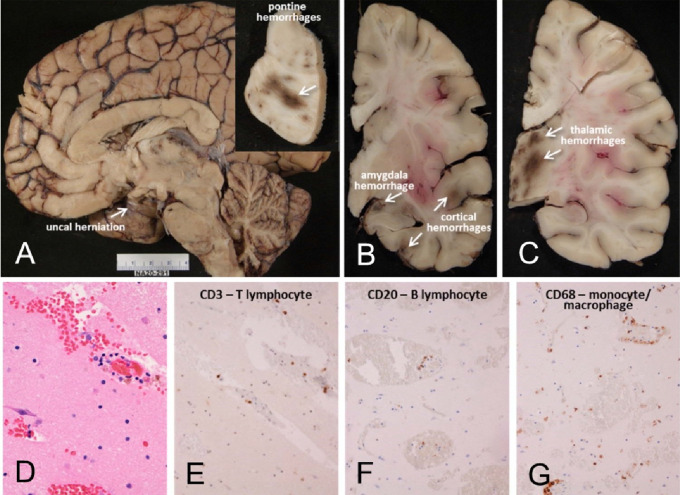
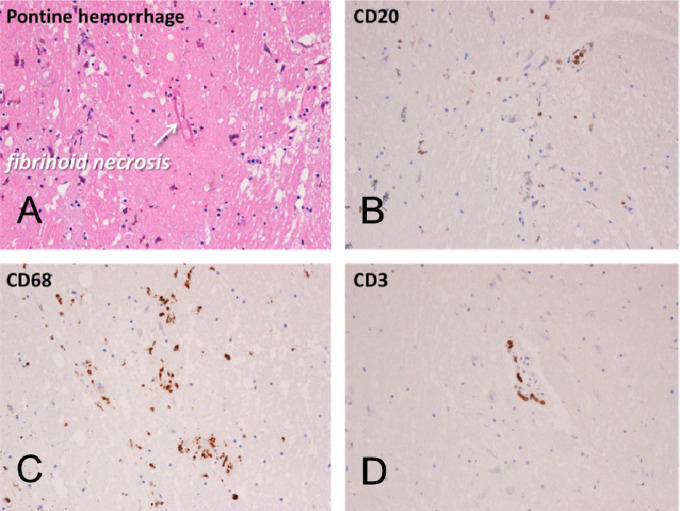
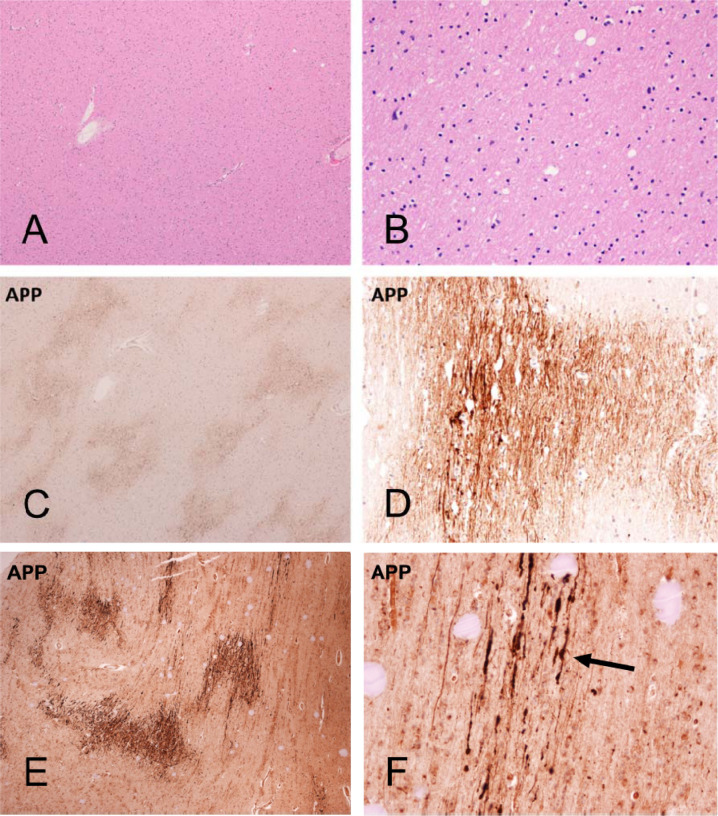
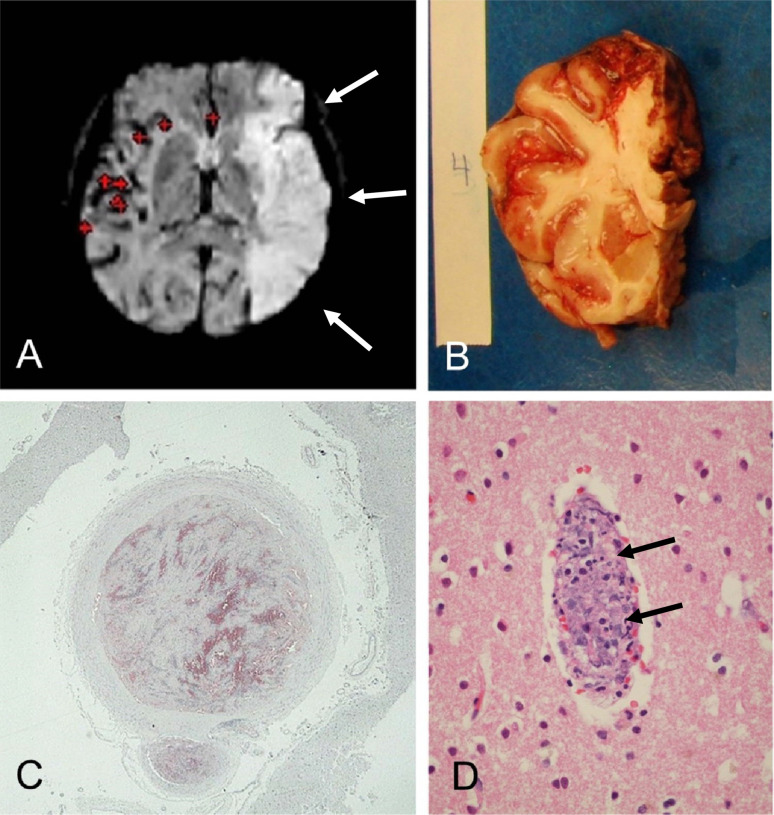
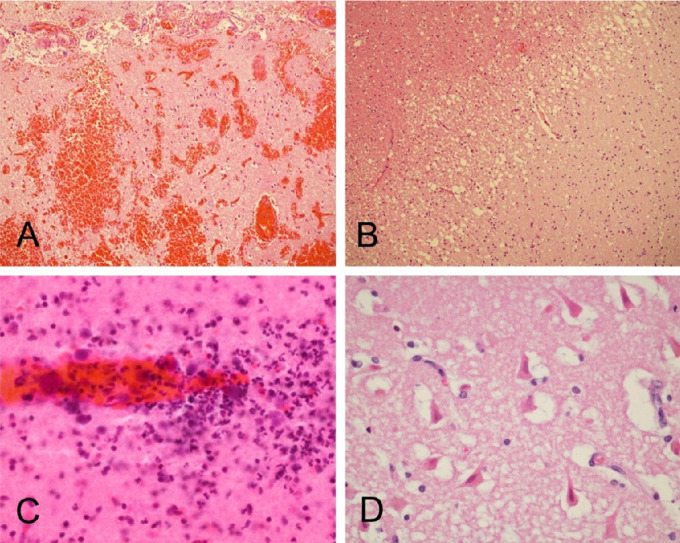
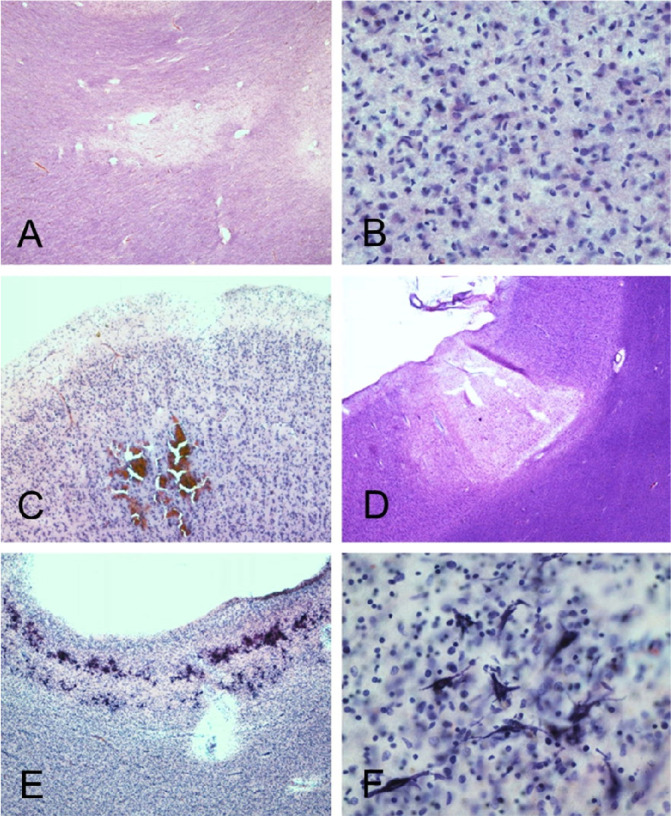
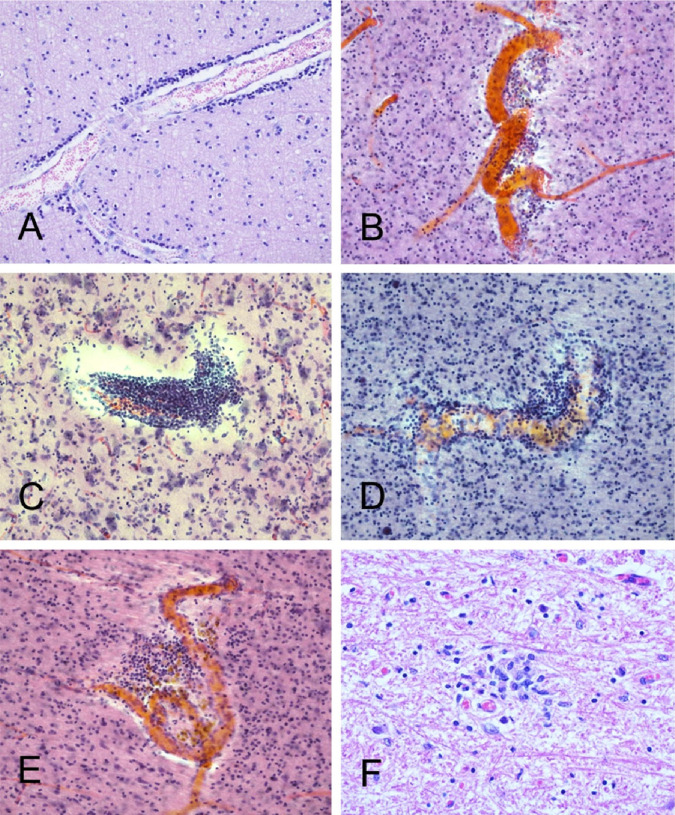
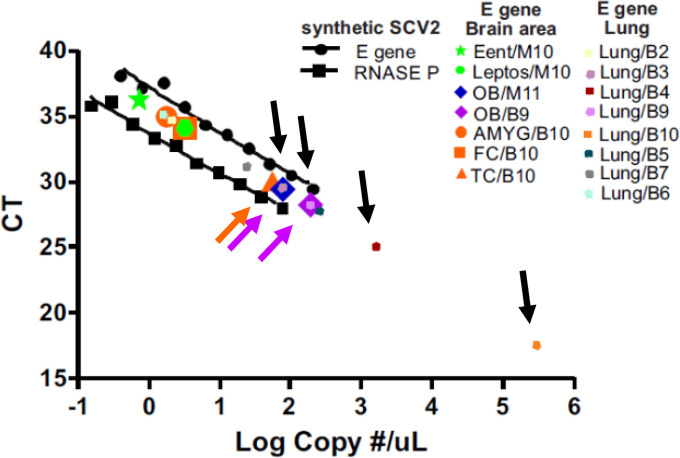
The coronavirus SARS-CoV-2 (SCV2) causes acute respiratory distress, termed COVID-19 disease, with substantial morbidity and mortality. As SCV2 is related to previously-studied coronaviruses that have been shown to have the capability for brain invasion, it seems likely that SCV2 may be able to do so as well. To date, although there have been many clinical and autopsy-based reports that describe a broad range of SCV2-associated neurological conditions, it is unclear what fraction of these have been due to direct CNS invasion versus indirect effects caused by systemic reactions to critical illness. Still critically lacking is a comprehensive tissue-based survey of the CNS presence and specific neuropathology of SCV2 in humans. We conducted an extensive neuroanatomical survey of RT-PCR-detected SCV2 in 16 brain regions from 20 subjects who died of COVID-19 disease. Targeted areas were those with cranial nerve nuclei, including the olfactory bulb, medullary dorsal motor nucleus of the vagus nerve and the pontine trigeminal nerve nuclei, as well as areas possibly exposed to hematogenous entry, including the choroid plexus, leptomeninges, median eminence of the hypothalamus and area postrema of the medulla. Subjects ranged in age from 38 to 97 (mean 77) with 9 females and 11 males. Most subjects had typical age-related neuropathological findings. Two subjects had severe neuropathology, one with a large acute cerebral infarction and one with hemorrhagic encephalitis, that was unequivocally related to their COVID-19 disease while most of the 18 other subjects had non-specific histopathology including focal β-amyloid precursor protein white matter immunoreactivity and sparse perivascular mononuclear cell cuffing. Four subjects (20%) had SCV2 RNA in one or more brain regions including the olfactory bulb, amygdala, entorhinal area, temporal and frontal neocortex, dorsal medulla and leptomeninges. The subject with encephalitis was SCV2-positive in a histopathologically-affected area, the entorhinal cortex, while the subject with the large acute cerebral infarct was SCV2-negative in all brain regions. Like other human coronaviruses, SCV2 can inflict acute neuropathology in susceptible patients. Much remains to be understood, including what viral and host factors influence SCV2 brain invasion and whether it is cleared from the brain subsequent to the acute illness.
Keywords: RT-PCR; coronavirus; encephalitis; hemorrhage; hypoxia; infarction; neuropathology.
Figures
Similar articles
-
SARS-CoV-2 infection alters mitochondrial and cytoskeletal function in human respiratory epithelial cells mediated by expression of spike protein.mBio. 2023 Aug 31;14(4):e0082023. doi: 10.1128/mbio.00820-23. Epub 2023 Jul 28. mBio. 2023. PMID: 37504520 Free PMC article.
-
Neuropathology of patients with COVID-19 in Germany: a post-mortem case series.Lancet Neurol. 2020 Nov;19(11):919-929. doi: 10.1016/S1474-4422(20)30308-2. Epub 2020 Oct 5. Lancet Neurol. 2020. PMID: 33031735 Free PMC article.
-
Neuropathological findings in two patients with fatal COVID-19.Neuropathol Appl Neurobiol. 2021 Feb;47(1):17-25. doi: 10.1111/nan.12662. Epub 2020 Sep 24. Neuropathol Appl Neurobiol. 2021. PMID: 32895961
-
Neurological manifestations associated with SARS-CoV-2 and other coronaviruses: A narrative review for clinicians.Rev Neurol (Paris). 2021 Jan-Feb;177(1-2):51-64. doi: 10.1016/j.neurol.2020.10.001. Epub 2020 Dec 16. Rev Neurol (Paris). 2021. PMID: 33446327 Free PMC article. Review.
-
Neurological manifestations of SARS-CoV-2: complexity, mechanism and associated disorders.Eur J Med Res. 2023 Aug 30;28(1):307. doi: 10.1186/s40001-023-01293-2. Eur J Med Res. 2023. PMID: 37649125 Free PMC article. Review.
Cited by
-
Biomedical Perspectives of Acute and Chronic Neurological and Neuropsychiatric Sequelae of COVID-19.Curr Neuropharmacol. 2022;20(6):1229-1240. doi: 10.2174/1570159X20666211223130228. Curr Neuropharmacol. 2022. PMID: 34951387 Free PMC article.
-
Neuropathological Aspects of SARS-CoV-2 Infection: Significance for Both Alzheimer's and Parkinson's Disease.Front Neurosci. 2022 May 3;16:867825. doi: 10.3389/fnins.2022.867825. eCollection 2022. Front Neurosci. 2022. PMID: 35592266 Free PMC article. Review.
-
The viral hypothesis in Alzheimer's disease: SARS-CoV-2 on the cusp.Front Aging Neurosci. 2023 Mar 15;15:1129640. doi: 10.3389/fnagi.2023.1129640. eCollection 2023. Front Aging Neurosci. 2023. PMID: 37009449 Free PMC article. Review.
-
Viral mapping in COVID-19 deceased in the Augsburg autopsy series of the first wave: A multiorgan and multimethodological approach.PLoS One. 2021 Jul 19;16(7):e0254872. doi: 10.1371/journal.pone.0254872. eCollection 2021. PLoS One. 2021. PMID: 34280238 Free PMC article.
-
Nervous System-Systemic Crosstalk in SARS-CoV-2/COVID-19: A Unique Dyshomeostasis Syndrome.Front Neurosci. 2021 Aug 27;15:727060. doi: 10.3389/fnins.2021.727060. eCollection 2021. Front Neurosci. 2021. PMID: 34512253 Free PMC article. Review.
References
-
- Baig AM, Khaleeq A, Ali U, et al. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host-Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem Neurosci. 2020; 11:995–998. - PubMed
-
- Lapina C, Rodic M, Pechanski D, et al. The potential genetic network of human brain SARS-CoV-2 infection. BIORXIV. 2020; 10.1101/2020.04.06.027318 - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous