

Diagnostic performance of preoperative [18F]FDG-PET/CT for lymph node staging in vulvar cancer: a large single-centre study
- PMID: 33619601
- PMCID: PMC8426310
- DOI: 10.1007/s00259-021-05257-8
Diagnostic performance of preoperative [18F]FDG-PET/CT for lymph node staging in vulvar cancer: a large single-centre study
Abstract
Purpose: This retrospective study aimed to assess the diagnostic performance of preoperative [18F]FDG-PET/CT in predicting the groin and pelvic lymph node (LN) status in a large single-centre series of vulvar cancer patients.
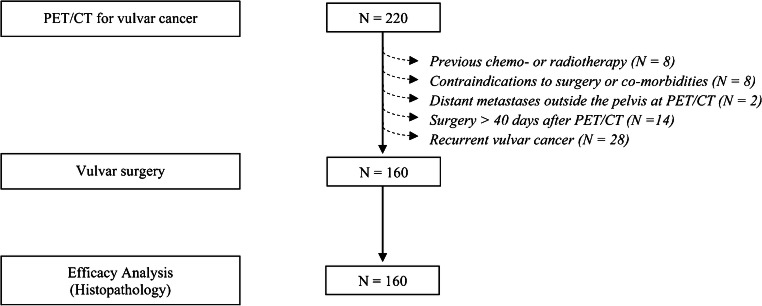
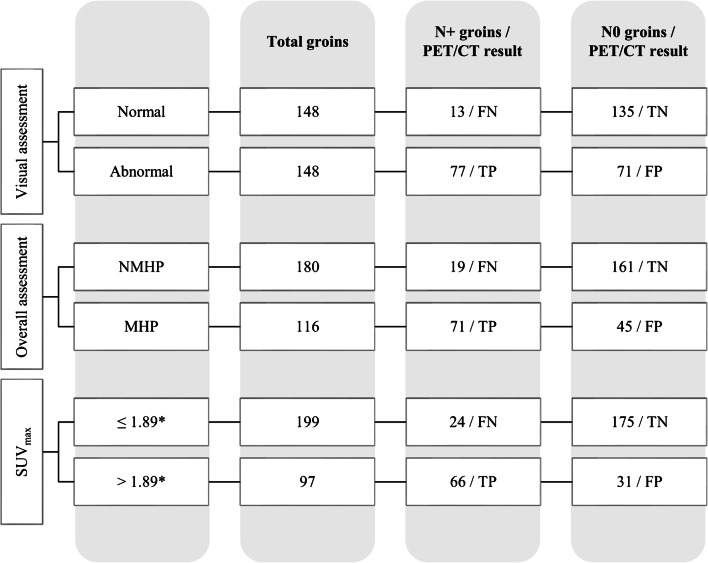
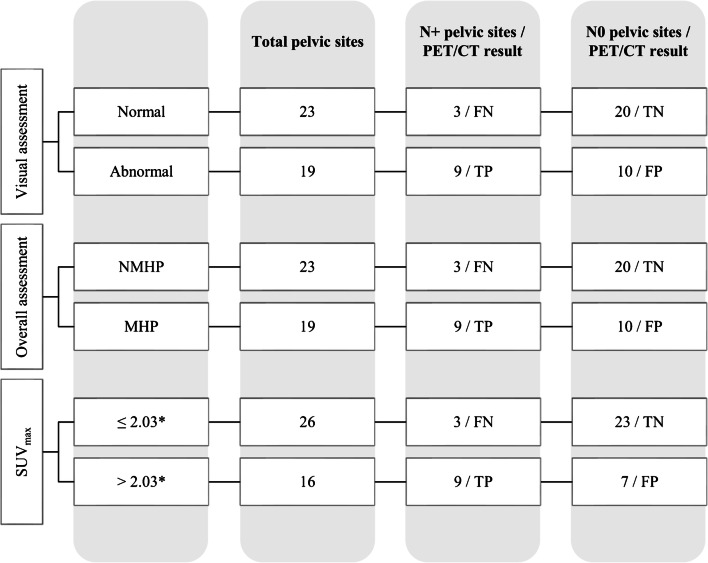
Methods: Between January 2013 and October 2018, among all consecutive women with proven vulvar cancer submitted to [18F]FDG-PET/CT, 160 patients were included. LNs were analysed by two qualitative methods assessing PET information (defined as visual assessment) and a combination of PET and low-dose CT information (defined as overall assessment), respectively, as well as semi-quantitative analysis (LN-SUVmax). Sensitivity, specificity, accuracy, positive and negative predictive values (PPV and NPV) in predicting the groin and pelvic LN status were calculated in the overall study population; a subset analysis of groin parameters in clinically/ultrasonography negative patients was also performed. Histopathology was the reference standard.
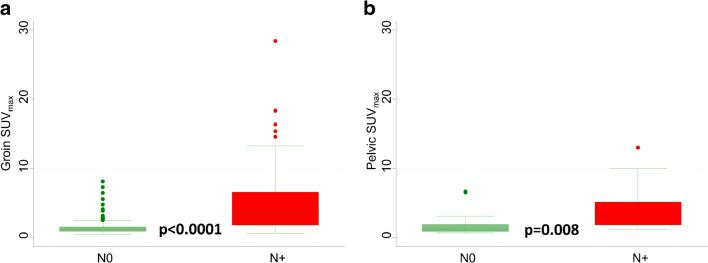
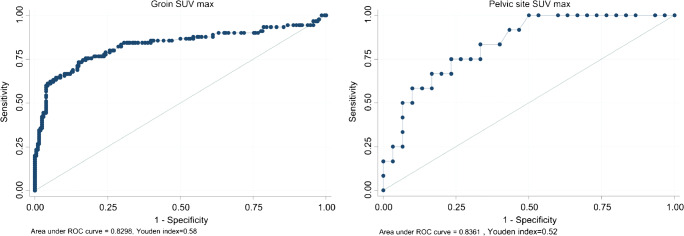
Results: All patients underwent vulvar and inguinofemoral LN surgery, and 35 pelvic LN surgery. Overall, 338 LN sites (296 groins and 42 pelvic sites) were histologically examined with 30.4% prevalence of metastatic groins and 28.6% for metastatic pelvic sites. In the overall study population, sensitivity (95% confidence interval, CI), specificity (95% CI), accuracy (95% CI), PPV (95% CI) and NPV (95% CI) at the groin level were 85.6% (78.3-92.8), 65.5% (59.0-72.0), 71.6% (66.5-76.8), 52.0% (44.0-60.1) and 91.2% (86.7-95.8) for visual assessment; 78.9% (70.5-87.3), 78.2% (72.5-83.8), 78.4% (73.7-83.1), 61.2% (52.3-70.1) and 89.4% (85.0-93.9) for overall assessment; and 73.3% (64.2-82.5), 85.0% (80.1-89.8), 81.4% (77.0-85.8), 68.0% (58.8-77.3) and 87.9% (83.4-92.5) for semi-quantitative analysis (SUVmax cut-off value 1.89 achieved by ROC analysis). Similar results were observed in the pelvis-based analysis.
Conclusion: In this large single-centre series of vulvar cancer patients, [18F]FDG-PET/CT showed good values of sensitivity and NPV in discriminating metastatic from non-metastatic LNs. In routine clinical practice, qualitative analysis is a reliable interpretative criterion making unnecessary commonly used semi-quantitative methods such as SUVmax.
Keywords: Lymph node staging; Personalized medicine; Vulvar cancer; [18F]FDG-PET/CT.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Comment in
-
Is it time to include [18F]FDG-PET/CT in the diagnostic work-up for lymph node staging in cN0 vulvar cancer patients?Eur J Nucl Med Mol Imaging. 2021 Sep;48(10):3043-3045. doi: 10.1007/s00259-021-05317-z. Eur J Nucl Med Mol Imaging. 2021. PMID: 33768280 No abstract available.
References
-
- National Cancer Institute. Cancer Stat Facts: Vulvar Cancer [Internet]. [access date 2021, Jan 03]. Available from: https://seer.cancer.gov/statfacts/html/vulva.html.
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN guidelines), Vulvar cancer (squamous cell carcinoma): version 2.2021 [access date 2021, Jan 03]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/vulvar.pdf.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
