

Surgical Impacts of Metastatic Non-small Cell Lung Cancer to the Thoracic and Lumbar Spine
- PMID: 33619918
- PMCID: PMC7900527
- DOI: 10.3346/jkms.2021.36.e52
Surgical Impacts of Metastatic Non-small Cell Lung Cancer to the Thoracic and Lumbar Spine
Abstract
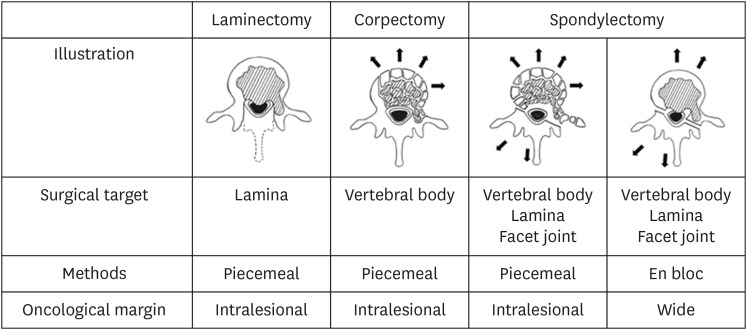
Background: Surgery for spinal metastasis is rapidly increasing in frequency with procedures ranging from laminectomy to spondylectomy combined with stabilization. This study investigated the effect of various surgical procedures for spinal metastasis of non-small cell lung cancer (NSCLC).
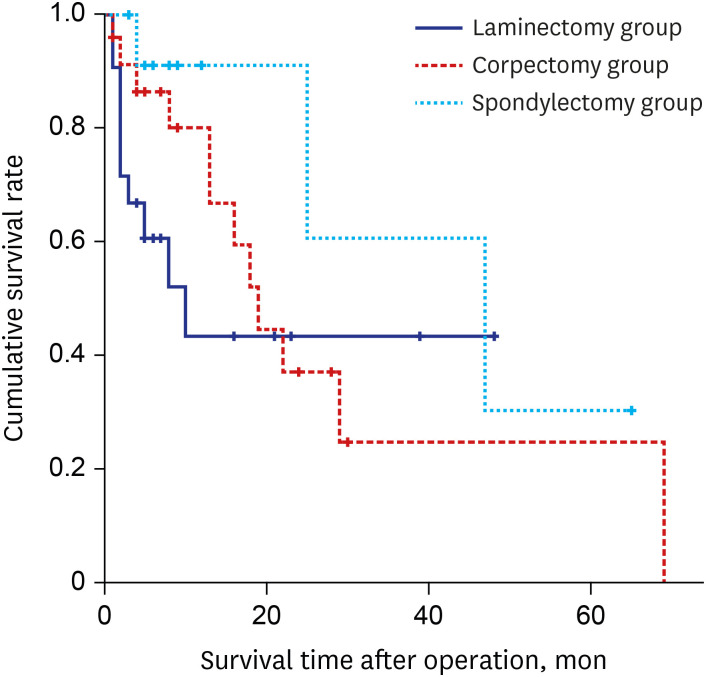
Methods: A single-center consecutive series of patients who underwent surgery for spinal metastasis of NSCLC were retrospectively reviewed. Patients' characteristics, radiographic parameters, operative data, clinical outcomes, and complications were analyzed. Surgical outcomes were assessed according to pain and performance status before and after surgery. Overall survival (OS) rate was estimated using the Kaplan-Meier method. Multivariate analysis was performed to detect factors independently associated with OS using a Cox proportional hazards model.
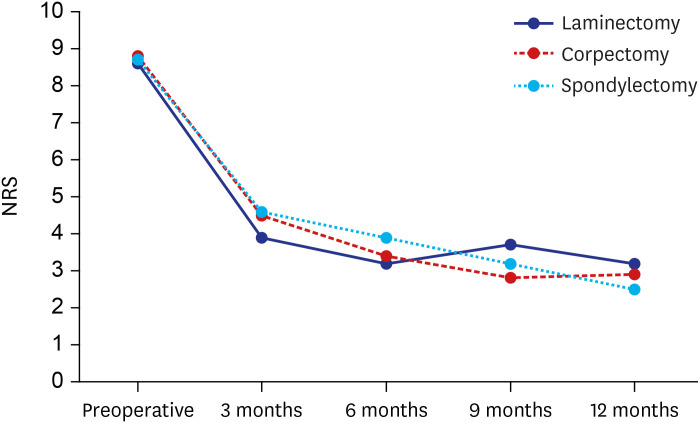
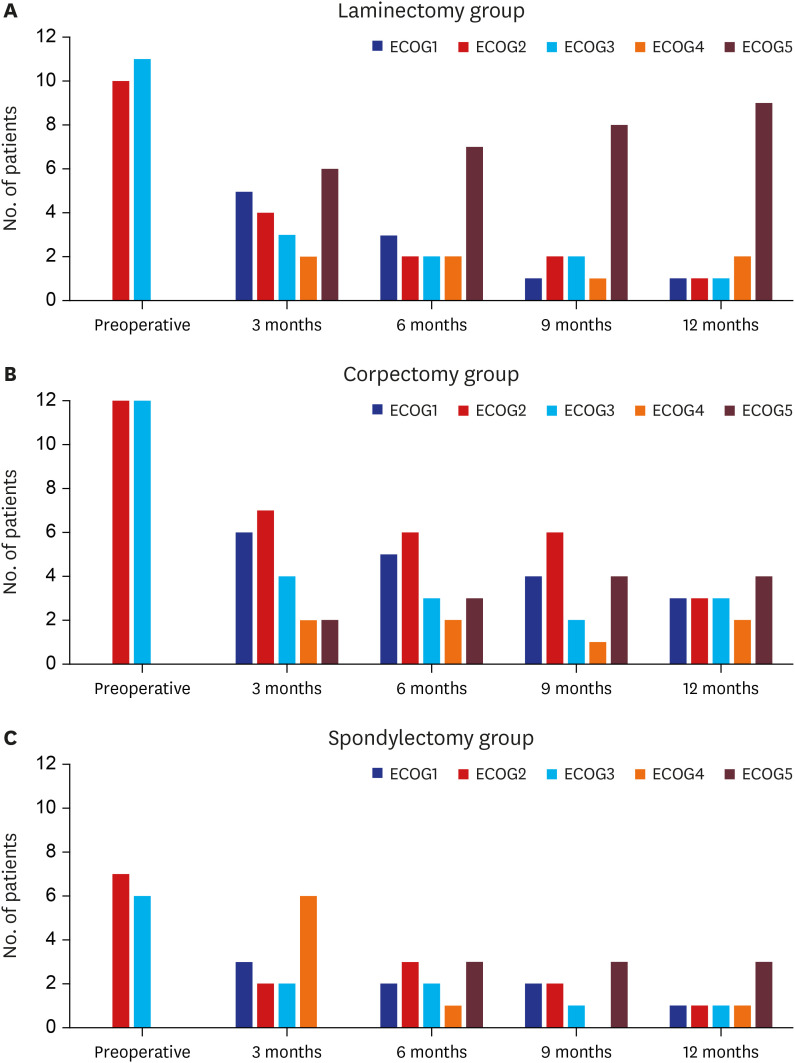
Results: Twenty-one patients were treated with laminectomy, 24 with corpectomy, 13 with spondylectomy (piecemeal or total en bloc fashion), and all procedures were combined with stabilization. Back pain and performance status improved significantly after surgical treatment among the three groups. Revision surgery due to tumor progression at the index level or spinal metastasis at another level were four patients (19.0%) in the laminectomy group, six patients (25.0%) in the corpectomy group, and one patient (7.7%) in the spondylectomy group. A Charlson comorbidity index and the number of spinal metastasis negatively affected OS (hazard ratio [HR], 19.613 and 2.244). Postoperative chemotherapy, time to metastasis, spondylectomy, and corpectomy had favorable associations with OS (HR, 0.455, 0.487, 0.619, and 0.715, respectively).
Conclusion: Postoperative chemotherapy was the most critical factor in OS of patients with metastatic NSCLC to the spine. An extensive surgical procedure (corpectomy/spondylectomy) with stabilization also could be beneficial for limited patients with spinal metastasis of NSCLC.
Keywords: Corpectomy; Laminectomy; Non-small Cell Lung Cancer; Overall Survival Rate; Spinal Metastasis; Spondylectomy.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
