

Sexual Assault and Carotid Plaque Among Midlife Women
- PMID: 33619993
- PMCID: PMC8174296
- DOI: 10.1161/JAHA.120.017629
Sexual Assault and Carotid Plaque Among Midlife Women
Abstract
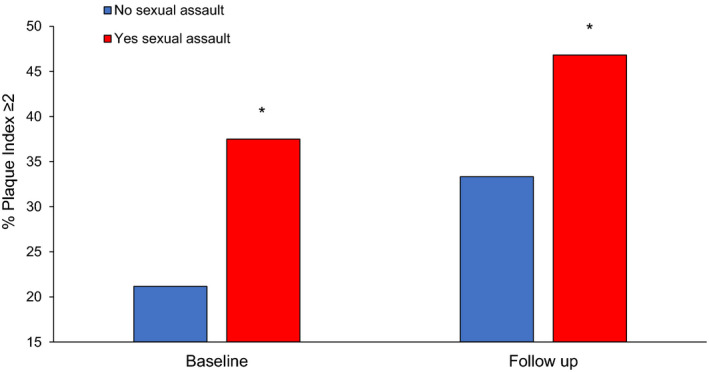
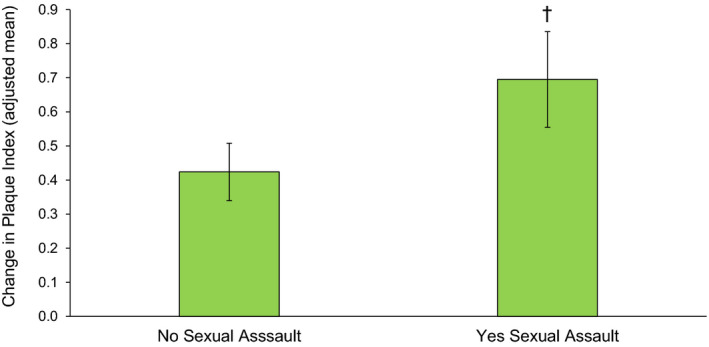
Background Sexual assault is a risk factor for poor mental health, yet its relationship to cardiovascular disease risk is not understood. We tested whether women with a sexual assault history had greater carotid atherosclerosis levels and progression over midlife. Methods and Results A total of 169 non-smoking, cardiovascular disease-free women aged 40 to 60 years were assessed twice over 5 years. At each point, women completed questionnaires, physical measures, phlebotomy, and carotid ultrasounds. Associations between sexual assault and carotid plaque level (score 0, 1, ≥2) and progression (score change) were assessed in multinomial logistic and linear regression models, adjusted for age, race/ethnicity, education, body mass index, blood pressure, lipids, insulin resistance, and additionally depression/post-traumatic stress symptoms; 28% of the women reported a sexual assault history. Relative to non-exposed women, women with a sexual assault history had an over 4-fold odds of a plaque score of ≥2 at baseline (≥2, odds ratio [OR] [95% CI]=4.35 [1.48-12.79], P=0.008; 1, OR [95% CI]=0.49 [0.12-1.97], P=0.32, versus no plaque; multivariable); and an over 3-fold odds of plaque ≥2 at follow-up (≥2, OR [95% CI]=3.65 [1.40-9.51], P=0.008; 1, OR [95% CI]=1.52 [0.46-4.99], P=0.49, versus no plaque; multivariable). Women with a sexual assault history also had an over 3-folds greater odds of a plaque score progression of ≥2 (OR [95% CI]=3.48[1.11-10.93], P=0.033, multivariable). Neither depression nor post-traumatic symptoms were related to plaque. Conclusions Sexual assault is associated with greater carotid atherosclerosis level and progression over midlife. Associations were not explained by standard cardiovascular disease risk factors. Future work should consider whether sexual assault prevention reduces women's cardiovascular disease risk.
Keywords: carotid atherosclerosis; psychological trauma; sexual violence; women's health.
Conflict of interest statement
Dr. Thurston reports personal fees from Astellas, Pfizer, Procter & Gamble, and Virtue Health, that are unrelated to the submitted work. Dr. Maki reports personal fees from Abbvie, Pfizer, and Balchem, that are unrelated to the submitted work. The remaining authors have no disclosures to report.
Figures
Similar articles
-
Trauma and its implications for women's cardiovascular health during the menopause transition: Lessons from MsHeart/MsBrain and SWAN studies.Maturitas. 2024 Apr;182:107915. doi: 10.1016/j.maturitas.2024.107915. Epub 2024 Jan 20. Maturitas. 2024. PMID: 38280354 Free PMC article. Review.
-
Association of Sexual Harassment and Sexual Assault With Midlife Women's Mental and Physical Health.JAMA Intern Med. 2019 Jan 1;179(1):48-53. doi: 10.1001/jamainternmed.2018.4886. JAMA Intern Med. 2019. PMID: 30285071 Free PMC article.
-
Exposure to Violence and Carotid Artery Intima-Media Thickness in Mexican Women.J Am Heart Assoc. 2017 Aug 17;6(8):e006249. doi: 10.1161/JAHA.117.006249. J Am Heart Assoc. 2017. PMID: 28862944 Free PMC article.
-
The Cardiovascular Cost of Silence: Relationships Between Self-silencing and Carotid Atherosclerosis in Midlife Women.Ann Behav Med. 2022 Mar 1;56(3):282-290. doi: 10.1093/abm/kaab046. Ann Behav Med. 2022. PMID: 34124743 Free PMC article.
-
A review of the health effects of sexual assault on African American women and adolescents.J Obstet Gynecol Neonatal Nurs. 2013 May-Jun;42(3):249-73. doi: 10.1111/1552-6909.12041. J Obstet Gynecol Neonatal Nurs. 2013. PMID: 23682695 Review.
Cited by
-
The Interplay between Child Maltreatment and Stressful Life Events during Adulthood and Cardiovascular Problems-A Representative Study.J Clin Med. 2021 Aug 31;10(17):3937. doi: 10.3390/jcm10173937. J Clin Med. 2021. PMID: 34501385 Free PMC article.
-
Interpersonal Trauma and Risk of Incident Cardiovascular Disease Events Among Women.J Am Heart Assoc. 2022 Apr 5;11(7):e024724. doi: 10.1161/JAHA.121.024724. Epub 2022 Mar 24. J Am Heart Assoc. 2022. PMID: 35322675 Free PMC article.
-
Everyday discrimination and subclinical indicators of stroke in midlife women.J Behav Med. 2025 Aug;48(4):583-593. doi: 10.1007/s10865-025-00568-9. Epub 2025 May 1. J Behav Med. 2025. PMID: 40310601
-
Trauma and its implications for women's cardiovascular health during the menopause transition: Lessons from MsHeart/MsBrain and SWAN studies.Maturitas. 2024 Apr;182:107915. doi: 10.1016/j.maturitas.2024.107915. Epub 2024 Jan 20. Maturitas. 2024. PMID: 38280354 Free PMC article. Review.
-
Sexual Violence and Risk of Hypertension in Women in the Nurses' Health Study II: A 7-Year Prospective Analysis.J Am Heart Assoc. 2022 Mar;11(5):e023015. doi: 10.1161/JAHA.121.023015. Epub 2022 Feb 22. J Am Heart Assoc. 2022. PMID: 35189695 Free PMC article.
References
-
- Smith SG, Zhang X, Basile KC, Merrick MT, Wang J, Kresnow M, Chen J. The National Intimate Partner And Sexual Violence Survey (NISVS): 2015 Data Brief—Updated Release. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2018:1–25.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
