

Variability in grading of ductal carcinoma in situ among an international group of pathologists
- PMID: 33620141
- PMCID: PMC8073001
- DOI: 10.1002/cjp2.201
Variability in grading of ductal carcinoma in situ among an international group of pathologists
Abstract
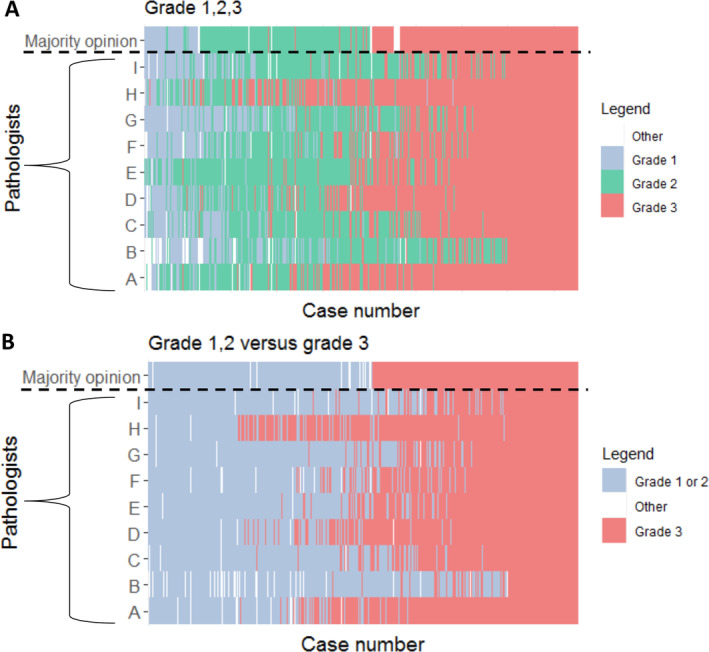
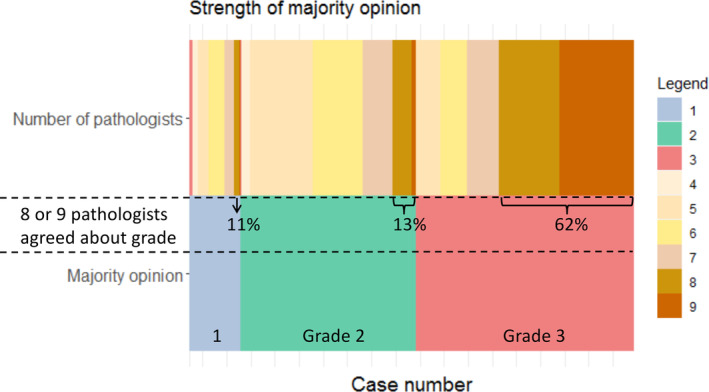
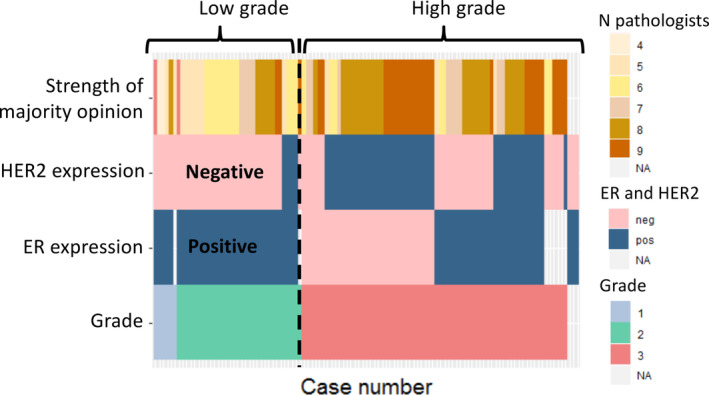
The prognostic value of cytonuclear grade in ductal carcinoma in situ (DCIS) is debated, partly due to high interobserver variability and the use of multiple guidelines. The aim of this study was to evaluate interobserver agreement in grading DCIS between Dutch, British, and American pathologists. Haematoxylin and eosin-stained slides of 425 women with primary DCIS were independently reviewed by nine breast pathologists based in the Netherlands, the UK, and the USA. Chance-corrected kappa (κma ) for association between pathologists was calculated based on a generalised linear mixed model using the ordinal package in R. Overall κma for grade of DCIS (low, intermediate, or high) was estimated to be 0.50 (95% confidence interval [CI] 0.44-0.56), indicating a moderate association between pathologists. When the model was adjusted for national guidelines, the association for grade did not change (κma = 0.53; 95% CI 0.48-0.57); subgroup analysis for pathologists using the UK pathology guidelines only had significantly higher association (κma = 0.58; 95% CI 0.56-0.61). To assess if concordance of grading relates to the expression of the oestrogen receptor (ER) and HER2, archived immunohistochemistry was analysed on a subgroup (n = 106). This showed that non-high grade according to the majority opinion was associated with ER positivity and HER2 negativity (100 and 89% of non-high grade cases, respectively). In conclusion, DCIS grade showed only moderate association using whole slide images scored by nine breast pathologists. As therapeutic decisions and inclusion in ongoing clinical trials are guided by DCIS grade, there is a pressing need to reduce interobserver variability in grading. ER and HER2 might be supportive to prevent the accidental and unwanted inclusion of high-grade DCIS in such trials.
Keywords: ductal carcinoma in situ; grade; interobserver variability; pathology.
© 2021 The Authors. The Journal of Pathology: Clinical Research published by The Pathological Society of Great Britain and Ireland & John Wiley & Sons, Ltd.
Figures
References
-
- Schuh F, Biazús JV, Resetkova E, et al. Reproducibility of three classification systems of ductal carcinoma in situ of the breast using a web‐based survey. Pathol Res Pract 2010; 206: 705–711. - PubMed
-
- Thompson AM, Clements K, Cheung S, et al. Management and 5‐year outcomes in 9938 women with screen‐detected ductal carcinoma in situ: the UK Sloane Project on behalf of the Sloane Project Steering Group (NHS Prospective Study of Screen‐Detected Non‐Invasive Neoplasias) 1. Eur J Cancer 2018; 101: 210–219. - PubMed
-
- Bijker N, Peterse JL, Duchateau L, et al. Risk factors for recurrence and metastasis after breast‐conserving therapy for ductal carcinoma‐in‐situ: analysis of European Organization for Research and Treatment of Cancer Trial 10853. J Clin Oncol 2001; 19: 2263–2271. - PubMed
-
- Elshof LE, Schaapveld M, Schmidt MK, et al. Subsequent risk of ipsilateral and contralateral invasive breast cancer after treatment for ductal carcinoma in situ: incidence and the effect of radiotherapy in a population‐based cohort of 10,090 women. Breast Cancer Res Treat 2016; 159: 553–563. - PMC - PubMed
-
- Visser LL, Elshof LE, Van de Vijver K, et al. Discordant marker expression between invasive breast carcinoma and corresponding synchronous and preceding DCIS. Am J Surg Pathol 2019; 43: 1574–1582. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
