

H3.3 K36M Mutation as a Clinical Diagnosis Method of Suspected Chondroblastoma Cases
- PMID: 33620145
- PMCID: PMC7957386
- DOI: 10.1111/os.12878
H3.3 K36M Mutation as a Clinical Diagnosis Method of Suspected Chondroblastoma Cases
Abstract
Objective: Whether H3.3 K36M mutation (H3K36M) could be an approach if the diagnosis of chondroblastoma (CB) patients was indistinct and it was suspected to be unclear clinically.
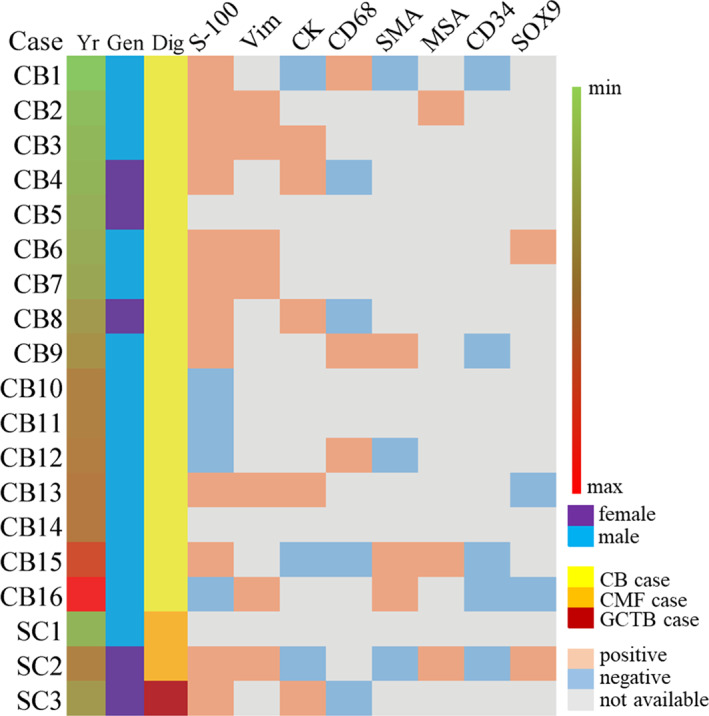
Methods: We reviewed and compared our clinical experiences of CB cases and some suspected cases, which were not diagnosed distinctly, between 2013 to 2019. A total of 15 male and four female cases included in this study were seperated into two groups, CB group and suspected case (SC) group. The CB group included 13 men and 3 women, with an age range from 9 to 54 (mean age, 22 years old). The SC group included two men and one woman, with the age range from 13 to 25 (mean age, 19 years old). In both groups the patients had been followed-up until December 2019 and none of the patients had prior treatment history. We evaluated the clinical complaints, radiological features, and clinical-histological features of the cases and performed an immunohistochemical (IHC) study to detect whether the H3K36M expression of cases was different, consistent with a gene-mutation analysis.
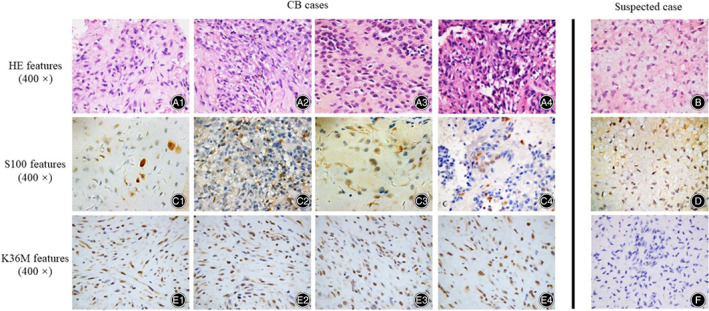
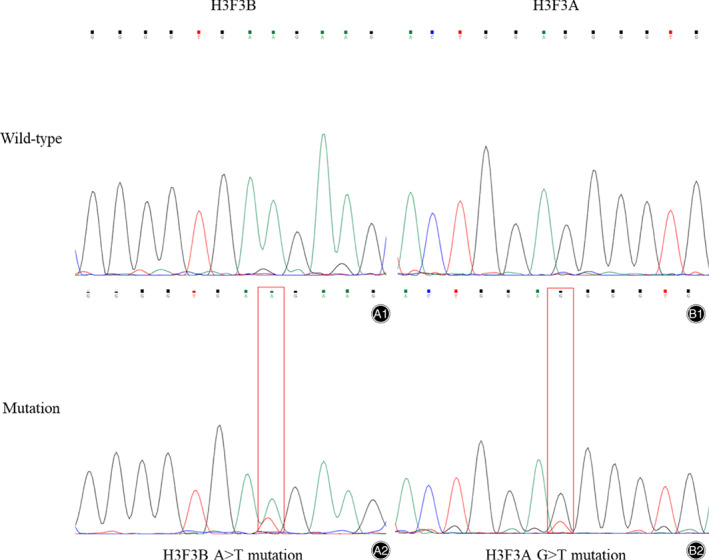
Results: In both groups, the radiologic features of both groups appeared as round low-density shadow with a clear edge, pathologic features showed diffuse proliferation of neoplastic cells with multinuclear giant cells. The radiological tumor size of CB group and SC group showed little difference, which was about 29.0*21.6 mm. Clinical-immunohistochemical features of both groups showed chondroid matrix inside with naïve tumor cells, multinucleated giant cells, and ground substance cells. Most of them showed chondro-related antibody positive (12 cases) but some of them showed S-100 negative (four cases). The clear difference of both groups was the result of H3K36M IHC study and gene analysis. In our cases, the CB group showed diffuse H3K36M positive and the SC group showed negative. The gene mutation analysis revealed that H3K36M-positive CB patients had K36M mutation, which were not found in the SC group. Sanger sequencing showed an A > T substitution at codon 36 of histone H3F3B. No other types of histone H3 mutation was detected in the CB group. Particularly, one of the suspected cases showed a G34W mutation was confirmed to be a giant cell tumor of bone (GCTB).
Conclusions: Our study showed H3K36M immunohistochemistry and gene mutation analysis were specific clinical diagnostic tools to distinguish suspected CB from other giant cell-rich or cartilage matrix-diffuse bone tumors. The clinical-radiological and histomorphological features of patients gave suggestions on whether the H3K36M IHC and gene analysis should be required.
Keywords: Chondroblastoma; Chondromyxoid fibroma; Giant-cell tumor of bone; Histone H3K36 mutation; Immunohistochemistry.
© 2021 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures

Similar articles
-
Immunohistochemistry for histone H3G34W and H3K36M is highly specific for giant cell tumor of bone and chondroblastoma, respectively, in FNA and core needle biopsy.Cancer Cytopathol. 2018 Aug;126(8):552-566. doi: 10.1002/cncy.22000. Epub 2018 May 14. Cancer Cytopathol. 2018. PMID: 29757500 Free PMC article.
-
Histone H3K36M mutation and trimethylation patterns in chondroblastoma.Histopathology. 2019 Jan;74(2):291-299. doi: 10.1111/his.13725. Epub 2018 Nov 4. Histopathology. 2019. PMID: 30098026 Free PMC article.
-
Mutation Analysis of H3F3A and H3F3B as a Diagnostic Tool for Giant Cell Tumor of Bone and Chondroblastoma.Am J Surg Pathol. 2015 Nov;39(11):1576-83. doi: 10.1097/PAS.0000000000000512. Am J Surg Pathol. 2015. PMID: 26457357
-
Chondroblastoma of foot bones; a clinicopathological study of 29 cases confirming the diagnostic utility of H3K36M and H3G34W antibodies at an uncommon site.Ann Diagn Pathol. 2023 Aug;65:152135. doi: 10.1016/j.anndiagpath.2023.152135. Epub 2023 Apr 7. Ann Diagn Pathol. 2023. PMID: 37075609 Review.
-
Chondroblastoma: An Update.Arch Pathol Lab Med. 2017 Jun;141(6):867-871. doi: 10.5858/arpa.2016-0281-RS. Arch Pathol Lab Med. 2017. PMID: 28557595 Review.
Cited by
-
Metaphyseal chondroblastoma in a pediatric patient.Radiol Case Rep. 2023 Jan 12;18(3):1210-1216. doi: 10.1016/j.radcr.2022.12.065. eCollection 2023 Mar. Radiol Case Rep. 2023. PMID: 36660567 Free PMC article.
-
Methionine intervention induces PD-L1 expression to enhance the immune checkpoint therapy response in MTAP-deleted osteosarcoma.Cell Rep Med. 2025 Mar 18;6(3):101977. doi: 10.1016/j.xcrm.2025.101977. Epub 2025 Feb 20. Cell Rep Med. 2025. PMID: 39983717 Free PMC article.
-
Roles of Histone H2B, H3 and H4 Variants in Cancer Development and Prognosis.Int J Mol Sci. 2024 Sep 7;25(17):9699. doi: 10.3390/ijms25179699. Int J Mol Sci. 2024. PMID: 39273649 Free PMC article. Review.
-
Disrupting YAP1-mediated glutamine metabolism induces synthetic lethality alongside ODC1 inhibition in osteosarcoma.Cell Oncol (Dordr). 2024 Oct;47(5):1845-1861. doi: 10.1007/s13402-024-00967-1. Epub 2024 Aug 8. Cell Oncol (Dordr). 2024. PMID: 39115605
-
Comparative analysis of X-ray, CT, and MRI images in patients with chondroblastoma in tubular and non-tubular bones.J Bone Oncol. 2025 May 28;52:100691. doi: 10.1016/j.jbo.2025.100691. eCollection 2025 Jun. J Bone Oncol. 2025. PMID: 40521137 Free PMC article.
References
-
- Qasem SA, DeYoung BR. Cartilage‐forming tumors. Semin Diagn Pathol, 2014, 31: 10–20. - PubMed
-
- Chen W, DiFrancesco LM. Chondroblastoma: an update. Arch Pathol Lab Med, 2017, 141: 867–871. - PubMed
-
- De Mattos CB, Angsanuntsukh C, Arkader A, Dormans JP. Chondroblastoma and chondromyxoid fibroma. J Am Acad Orthop Surg, 2013, 21: 225–233. - PubMed
-
- Kinkor Z, Grossmann P, Špůrková Z, Věcková Z, Matějovský Z. Chondroblastoma‐like primary malignant giant cell tumor of the humerus ‐ a case report. Cesk Patol, 2019, 55: 42–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
