

High population-attributable fractions of traditional risk factors for non-AIDS-defining diseases among people living with HIV in China: a cohort study
- PMID: 33620297
- PMCID: PMC7971336
- DOI: 10.1080/22221751.2021.1894904
High population-attributable fractions of traditional risk factors for non-AIDS-defining diseases among people living with HIV in China: a cohort study
Abstract
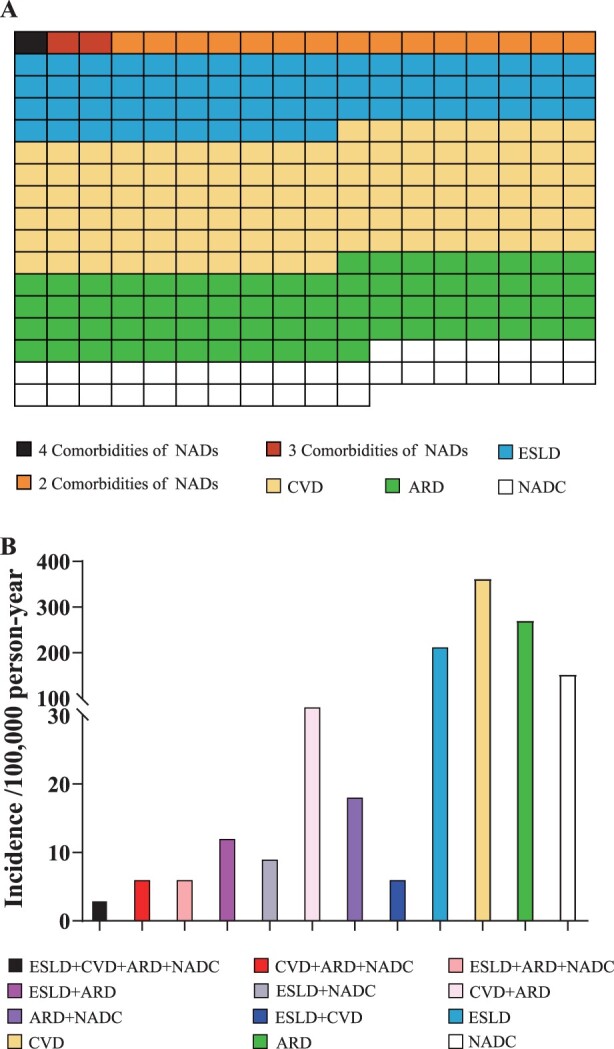
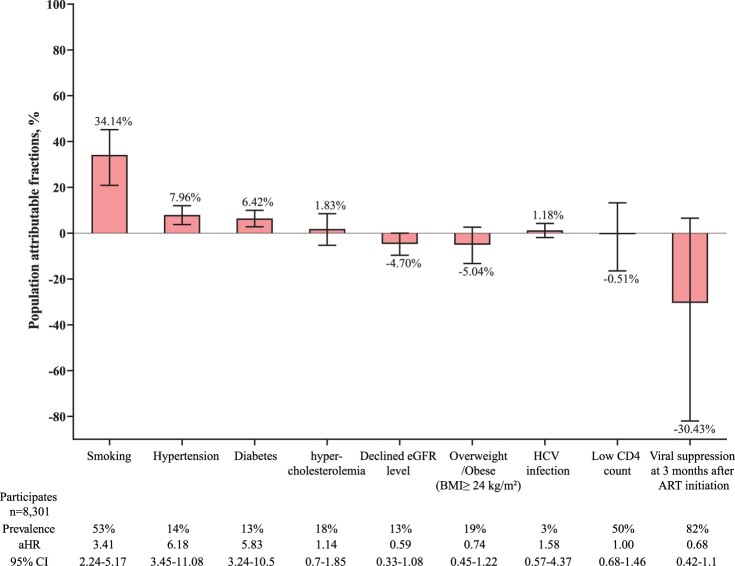
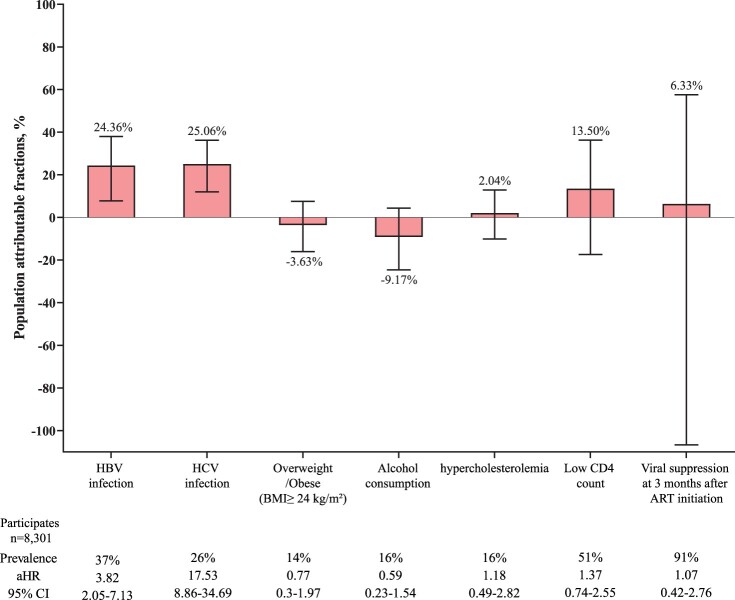
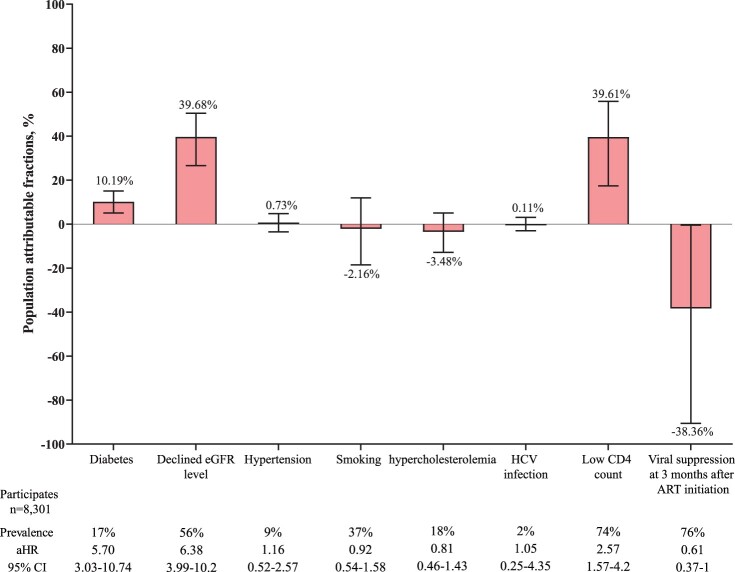
Morbidity and mortality of non-AIDS-defining diseases (NADs) have become the increasing burden of people living with HIV (PLWH) with long-term antiretroviral therapy (ART). We aimed to quantify the contribution of modifiable risk factors to NADs. We included PLWHs starting ART at the Third People's Hospital of Shenzhen (China) from Jan 1, 2010 to Dec 31, 2017. We defined NAD outcomes of interest as cardiovascular disease (CVD), end-stage liver disease (ESLD), advanced renal disease (ARD), and non-AIDS-defining cancers (NADCs). We estimated incidence of outcomes and population-attributable fractions (PAFs) of modifiable traditional and HIV-related risk factors for each outcome. Overall, 8,301 participants (median age at study entry, 31 years) contributed 33,146 person-years of follow-up (PYFU). Incidence of CVD (362/100,000 PYFU) was the highest among outcomes, followed by that of ARD (270/100,000 PYFU), ESLD (213/100,000 PYFU), and NADC (152/100,000 PYFU). Totally, 34.14% of CVD was attributable to smoking, 7.98% to hypertension, and 6.44% to diabetes. For ESLD, 24.57% and 25.04% of it could be avoided if chronic hepatitis B and C virus infection, respectively, did not present. The leading PAFs for ARD were declined estimated glomerular filtration rate (eGFR) (39.68%) and low CD4 count (39.61%), followed by diabetes (10.19%). PAFs of hypertension, diabetes, and smoking for CVD, and declined eGFR and diabetes for ARD increased with age. The contribution of traditional risk factors for these NADs far outweighed the HIV-related risk factors. Individual-level interventions and population-level policy-making is needed to focus on these factors to prevent NADs in long-term management of HIV infection.
Keywords: AIDS; Human immunodeficiency virus; incidence; non-AIDS-defining diseases; population attributable fraction.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
Similar articles
-
Contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the USA and Canada: a collaboration of cohort studies.Lancet HIV. 2019 Feb;6(2):e93-e104. doi: 10.1016/S2352-3018(18)30295-9. Epub 2019 Jan 22. Lancet HIV. 2019. PMID: 30683625 Free PMC article.
-
Serious clinical events in HIV-positive persons with chronic kidney disease.AIDS. 2019 Nov 15;33(14):2173-2188. doi: 10.1097/QAD.0000000000002331. AIDS. 2019. PMID: 31385862
-
Cancer-Attributable Mortality Among People With Treated Human Immunodeficiency Virus Infection in North America.Clin Infect Dis. 2017 Aug 15;65(4):636-643. doi: 10.1093/cid/cix392. Clin Infect Dis. 2017. PMID: 29017269 Free PMC article.
-
Higher cardiovascular disease risks in people living with HIV: A systematic review and meta-analysis.J Glob Health. 2024 Apr 26;14:04078. doi: 10.7189/jogh.14.04078. J Glob Health. 2024. PMID: 38666515 Free PMC article.
-
The Pattern of Non-AIDS-defining Cancers in the HIV Population: Epidemiology, Risk Factors and Prognosis. A Review.Curr HIV Res. 2019;17(1):1-12. doi: 10.2174/1570162X17666190327153038. Curr HIV Res. 2019. PMID: 30919779 Review.
Cited by
-
The prevalence of dyslipidemia and its correlation with anti-retroviral therapy among people living with HIV in China: a systematic review and meta-analysis.Front Cardiovasc Med. 2025 Jun 13;12:1498165. doi: 10.3389/fcvm.2025.1498165. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40585401 Free PMC article.
-
The Influencing Factors of HIV-Preventive Behavior Based on Health Belief Model among HIV-Negative MSMs in Western China: A Structural Equation Modeling Analysis.Int J Environ Res Public Health. 2022 Aug 17;19(16):10185. doi: 10.3390/ijerph191610185. Int J Environ Res Public Health. 2022. PMID: 36011822 Free PMC article.
-
Erythropoietin and iron for anemia in HIV-infected patients undergoing maintenance hemodialysis in China: a cross-sectional study.BMC Nephrol. 2022 Feb 8;23(1):60. doi: 10.1186/s12882-022-02693-y. BMC Nephrol. 2022. PMID: 35135490 Free PMC article.
-
A Prognostic Model to Assess Long-Term Survival of Patients on Antiretroviral Therapy: A 15-Year Retrospective Cohort Study in Southwestern China.Open Forum Infect Dis. 2021 Jun 12;8(7):ofab309. doi: 10.1093/ofid/ofab309. eCollection 2021 Jul. Open Forum Infect Dis. 2021. PMID: 34327255 Free PMC article.
-
Disparities in healthcare access and utilization among people living with HIV in China: a scoping review and meta-analysis.Res Sq [Preprint]. 2023 Apr 6:rs.3.rs-2744464. doi: 10.21203/rs.3.rs-2744464/v1. Res Sq. 2023. Update in: HIV Med. 2023 Nov;24(11):1093-1105. doi: 10.1111/hiv.13523. PMID: 37066259 Free PMC article. Updated. Preprint.
References
-
- Frank TD, Carter A, Jahagirdar D, et al. . Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the global burden of diseases, injuries, and risk factors study 2017. Lancet HIV. 2019;6(12):e831–e859. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous