

Incidence of major adverse cardiac events following non-cardiac surgery
- PMID: 33620378
- PMCID: PMC8245139
- DOI: 10.1093/ehjacc/zuaa008
Incidence of major adverse cardiac events following non-cardiac surgery
Abstract
Aims: Major adverse cardiac events (MACE) triggered by non-cardiac surgery are prognostically important perioperative complications. However, due to often asymptomatic presentation, the incidence and timing of postoperative MACE are incompletely understood.
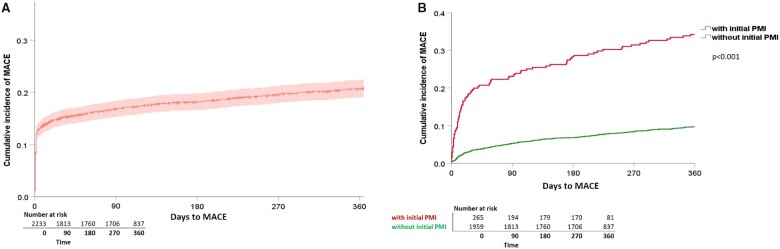
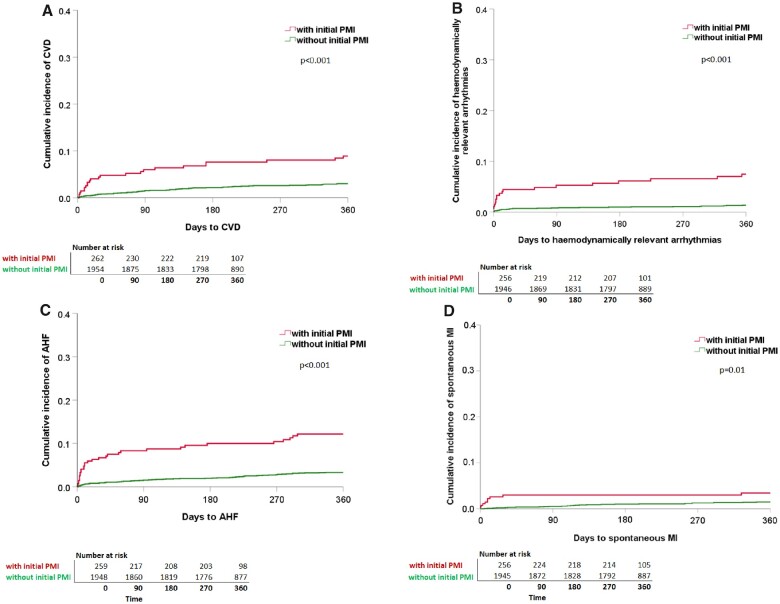
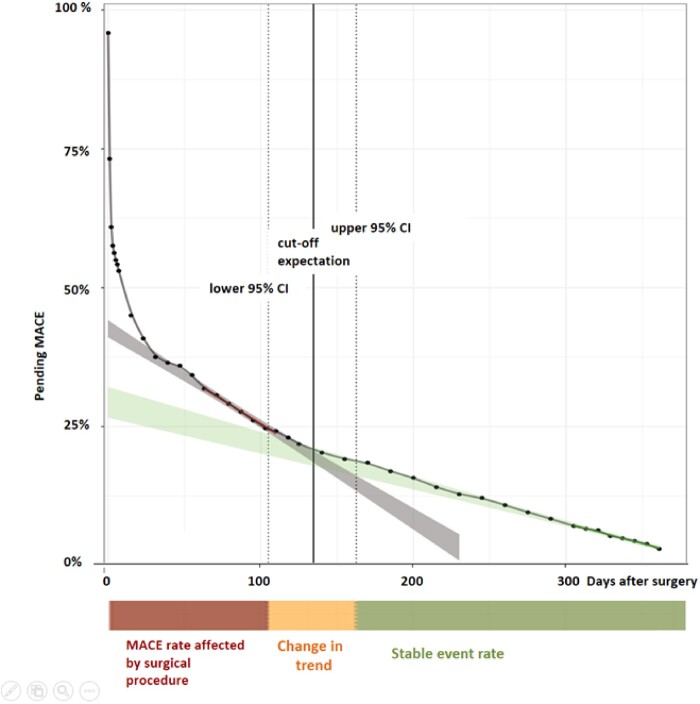
Methods and results: We conducted a prospective observational study implementing a perioperative screening for postoperative MACE [cardiovascular death (CVD), acute heart failure (AHF), haemodynamically relevant arrhythmias, spontaneous myocardial infarction (MI), and perioperative myocardial infarction/injury (PMI)] in patients at increased cardiovascular risk (≥65 years OR ≥45 years with history of cardiovascular disease) undergoing non-cardiac surgery at a tertiary hospital. All patients received serial measurements of cardiac troponin to detect asymptomatic MACE. Among 2265 patients (mean age 73 years, 43.4% women), the incidence of MACE was 15.2% within 30 days, and 20.6% within 365 days. CVD occurred in 1.2% [95% confidence interval (CI) 0.9-1.8] and in 3.7% (95% CI 3.0-4.5), haemodynamically relevant arrhythmias in 1.2% (95% CI 0.9-1.8) and in 2.1% (95% CI 1.6-2.8), AHF in 1.6% (95% CI 1.2-2.2) and in 4.2% (95% CI 3.4-5.1), spontaneous MI in 0.5% (95% CI 0.3-0.9) and in 1.6% (95% CI 1.2-2.2), and PMI in 13.2% (95% CI 11.9-14.7) and in 14.8% (95% CI 13.4-16.4) within 30 days and within 365 days, respectively. The MACE-incidence was increased above presumed baseline rate until Day 135 (95% CI 104-163), indicating a vulnerable period of 3-5 months.
Conclusion: One out of five high-risk patients undergoing non-cardiac surgery will develop one or more MACE within 365 days. The risk for MACE remains increased for about 5 months after non-cardiac surgery.
Trial registration: https://www.clinicaltrials.gov. Unique identifier: NCT02573532.
Keywords: Acute myocardial infarction; Arrhythmia; Death; Heart failure; Surgery.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, Fu R, Azad T, Chao TE, Berry WR, Gawande AA. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 2015;385:S11. - PubMed
-
- Devereaux PJ, Xavier D, Pogue J, Guyatt G, Sigamani A, Garutti I, Leslie K, Rao-Melacini P, Chrolavicius S, Yang H, Macdonald C, Avezum A, Lanthier L, Hu W, Yusuf S. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med 2011;154:523–528. - PubMed
-
- González-Tallada A, Borrell-Vega J, Coronado C, Morales P, Miguel M de, Ferreira-González I, Nadal M de. Myocardial injury after noncardiac surgery: incidence, predictive factors, and outcome in high-risk patients undergoing thoracic surgery: an observational study. J Cardiothorac Vasc Anesth 2019;34:426–432. - PubMed
-
- Mangano DT, Browner WS, Hollenberg M, Li J, Tateo IM.. Long-term cardiac prognosis following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA 1992;268:233–239. - PubMed
-
- Sabaté S, Mases A, Guilera N, Canet J, Castillo J, Orrego C, Sabaté A, Fita G, Parramón F, Paniagua P, Rodríguez A, Sabaté M, ANESCARDIOCAT Group B, Rivilla M, Gine M, Sadurni M, Fau M, Arroyo R, Rojo A, Pujol Rosa E, Rovira I, Alcon A, Lacambra M, Pi A, Campello D, Sierra P, Arnal A, Llorente C, Mazo V, Lopez S. Incidence and predictors of major perioperative adverse cardiac and cerebrovascular events in non-cardiac surgery. Br J Anaesth 2011;107:879–890. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
