

Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator- and Vasopressor-Free Days in Patients With Sepsis: The VICTAS Randomized Clinical Trial
- PMID: 33620405
- PMCID: PMC7903252
- DOI: 10.1001/jama.2020.24505
Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator- and Vasopressor-Free Days in Patients With Sepsis: The VICTAS Randomized Clinical Trial
Erratum in
-
Addition of Nonauthor Collaborator Names of the VICTAS Trial.JAMA. 2021 Sep 21;326(11):1072. doi: 10.1001/jama.2021.15080. JAMA. 2021. PMID: 34431980 Free PMC article. No abstract available.
Abstract
Importance: Sepsis is a common syndrome with substantial morbidity and mortality. A combination of vitamin C, thiamine, and corticosteroids has been proposed as a potential treatment for patients with sepsis.
Objective: To determine whether a combination of vitamin C, thiamine, and hydrocortisone every 6 hours increases ventilator- and vasopressor-free days compared with placebo in patients with sepsis.
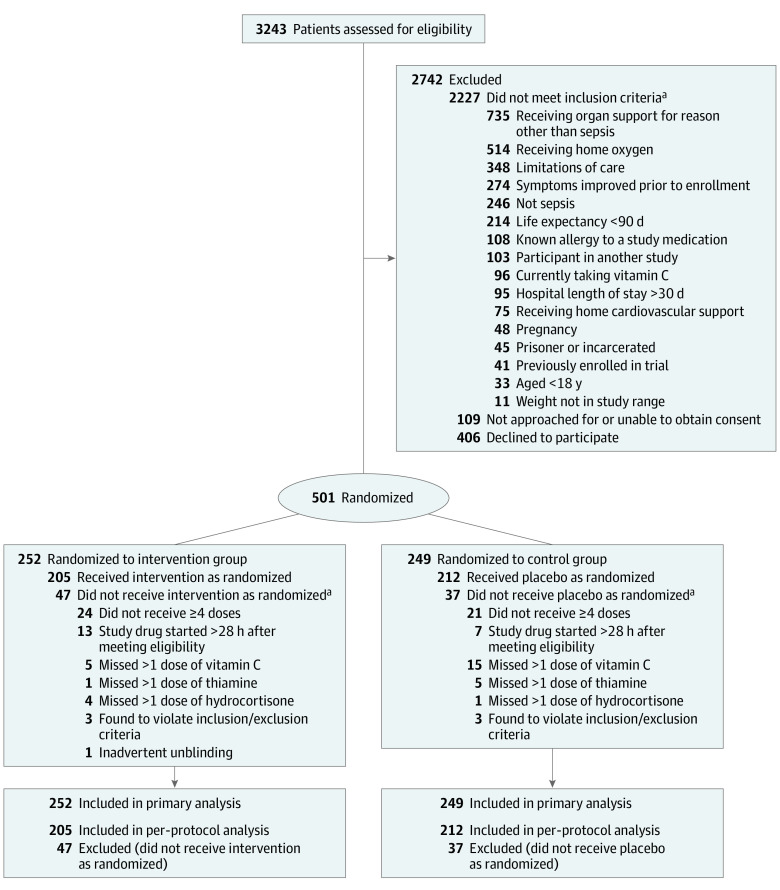
Design, setting, and participants: Multicenter, randomized, double-blind, adaptive-sample-size, placebo-controlled trial conducted in adult patients with sepsis-induced respiratory and/or cardiovascular dysfunction. Participants were enrolled in the emergency departments or intensive care units at 43 hospitals in the United States between August 2018 and July 2019. After enrollment of 501 participants, funding was withheld, leading to an administrative termination of the trial. All study-related follow-up was completed by January 2020.
Interventions: Participants were randomized to receive intravenous vitamin C (1.5 g), thiamine (100 mg), and hydrocortisone (50 mg) every 6 hours (n = 252) or matching placebo (n = 249) for 96 hours or until discharge from the intensive care unit or death. Participants could be treated with open-label corticosteroids by the clinical team, with study hydrocortisone or matching placebo withheld if the total daily dose was greater or equal to the equivalent of 200 mg of hydrocortisone.
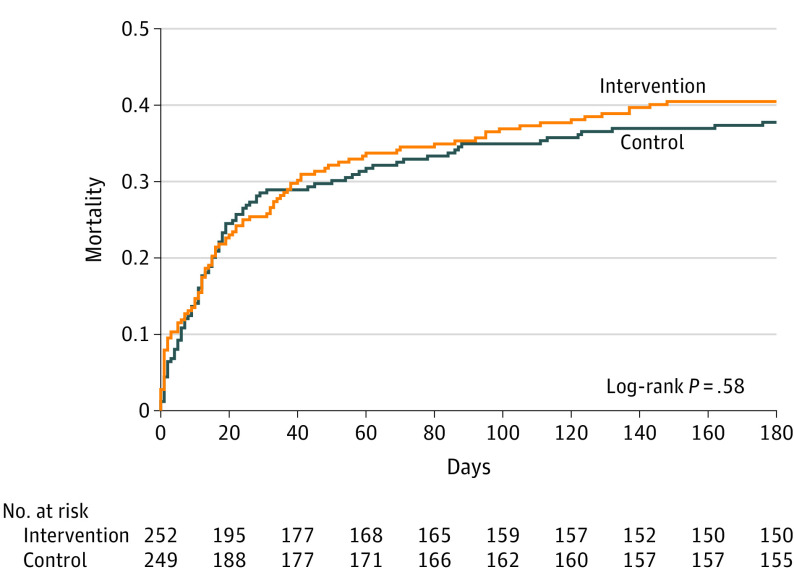
Main outcomes and measures: The primary outcome was the number of consecutive ventilator- and vasopressor-free days in the first 30 days following the day of randomization. The key secondary outcome was 30-day mortality.
Results: Among 501 participants randomized (median age, 62 [interquartile range {IQR}, 50-70] years; 46% female; 30% Black; median Acute Physiology and Chronic Health Evaluation II score, 27 [IQR, 20.8-33.0]; median Sequential Organ Failure Assessment score, 9 [IQR, 7-12]), all completed the trial. Open-label corticosteroids were prescribed to 33% and 32% of the intervention and control groups, respectively. Ventilator- and vasopressor-free days were a median of 25 days (IQR, 0-29 days) in the intervention group and 26 days (IQR, 0-28 days) in the placebo group, with a median difference of -1 day (95% CI, -4 to 2 days; P = .85). Thirty-day mortality was 22% in the intervention group and 24% in the placebo group.
Conclusions and relevance: Among critically ill patients with sepsis, treatment with vitamin C, thiamine, and hydrocortisone, compared with placebo, did not significantly increase ventilator- and vasopressor-free days within 30 days. However, the trial was terminated early for administrative reasons and may have been underpowered to detect a clinically important difference.
Trial registration: ClinicalTrials.gov Identifier: NCT03509350.
Conflict of interest statement
Figures
Comment in
-
Hydrocortisone, Vitamin C, and Thiamine for Treatment of Sepsis: Making Evidence Matter.JAMA. 2021 Feb 23;325(8):730-731. doi: 10.1001/jama.2020.26029. JAMA. 2021. PMID: 33620384 No abstract available.
-
Funding and DSMB Membership in the VICTAS Clinical Trial.JAMA. 2021 Feb 23;325(8):751-752. doi: 10.1001/jama.2020.25952. JAMA. 2021. PMID: 33620386 No abstract available.
-
[Focus general intensive care medicine. Intensive care studies from 2020/2021].Anaesthesist. 2021 Oct;70(10):888-894. doi: 10.1007/s00101-021-00976-x. Epub 2021 Jul 29. Anaesthesist. 2021. PMID: 34324037 Free PMC article. German. No abstract available.
References
-
- Torio CM, Moore BJ. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013 Agency for Healthcare Research and Quality; 2016. Healthcare Cost and Utilization Project Statistical Brief No. 204. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
