

The peak levels of highly sensitive troponin I predicts in-hospital mortality in COVID-19 patients with cardiac injury: a retrospective study
- PMID: 33620438
- PMCID: PMC7665398
- DOI: 10.1093/ehjacc/zuaa019
The peak levels of highly sensitive troponin I predicts in-hospital mortality in COVID-19 patients with cardiac injury: a retrospective study
Abstract
Aims: To investigate the association between levels of highly sensitive troponin I (hs-troponin I) and mortality in novel coronavirus disease 2019 (COVID-19) patients with cardiac injury.
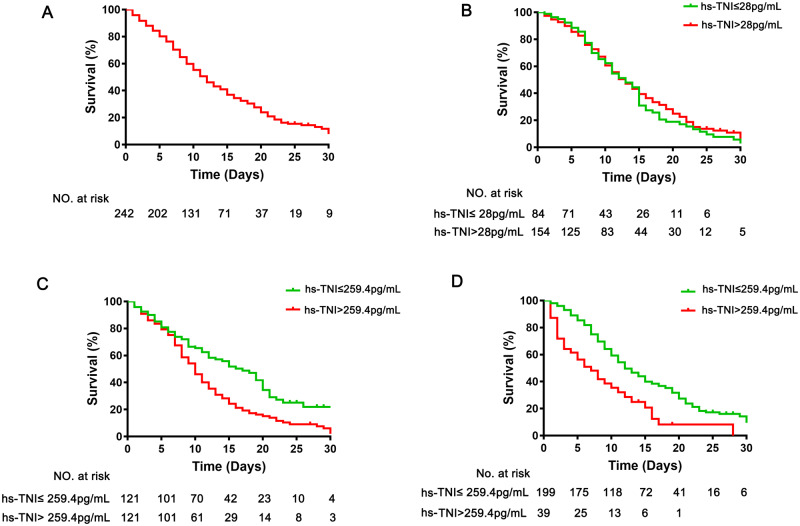
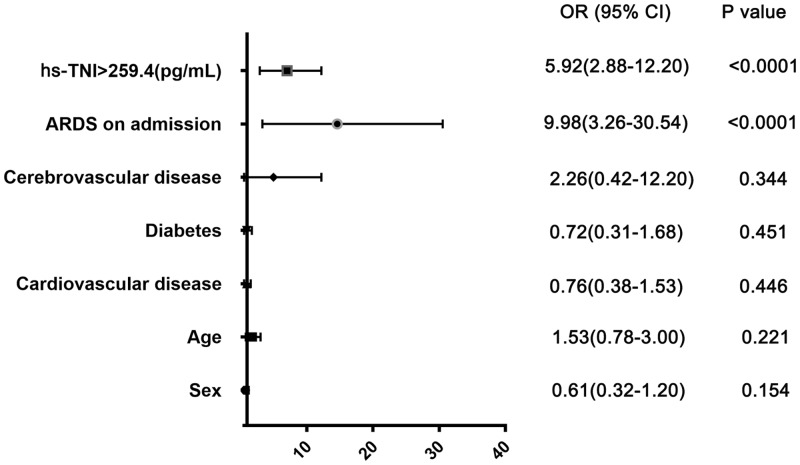
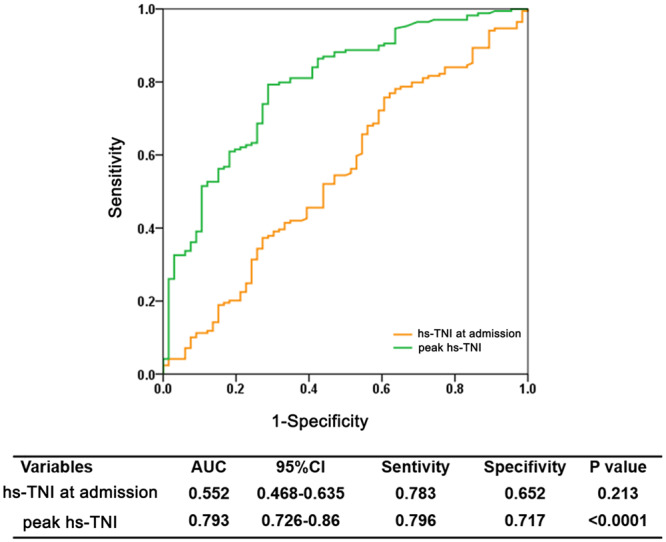
Methods and results: We retrospectively reviewed the medical records of all COVID-19 patients with increased levels of hs-troponin I from two hospitals in Wuhan, China. Demographic information, laboratory test results, cardiac ultrasonographic findings, and electrocardiograms were collected, and their predictive value on in-hospital mortality was explored using multivariable logistic regression. Of 1500 patients screened, 242 COVID-19 patients were enrolled in our study. Their median age was 68 years, and (48.8%) had underlying cardiovascular diseases. One hundred and seventy-six (72.7%) patients died during hospitalization. Multivariable logistic regression showed that C-reactive protein (>75.5 mg/L), D-dimer (>1.5 μg/mL), and acute respiratory distress syndrome were risk factors of mortality, and the peak hs-troponin I levels (>259.4 pg/mL) instead of the hs-troponin I levels at admission was predictor of death. The area under the receiver operating characteristic curve of the peak levels of hs-troponin I for predicting in-hospital mortality was 0.79 (95% confidence interval, 0.73-0.86; sensitivity, 0.80; specificity, 0.72; P < 0.0001).
Conclusion: Our results demonstrated that the risk of in-hospital death among COVID-19 patients with cardiac injury can be predicted by the peak levels of hs-troponin I during hospitalization and was significantly associated with oxygen supply-demand mismatch, inflammation, and coagulation.
Keywords: COVID-19; Cardiac injury; Levels of troponin I at admission; Mortality; Peak levels of troponin I.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Assessment of the Relationship between Mortality and Troponin I Levels in Hospitalized Patients with the Novel Coronavirus (COVID-19).Medicina (Kaunas). 2020 Dec 13;56(12):693. doi: 10.3390/medicina56120693. Medicina (Kaunas). 2020. PMID: 33322097 Free PMC article.
-
Longitudinal correlation of biomarkers of cardiac injury, inflammation, and coagulation to outcome in hospitalized COVID-19 patients.J Mol Cell Cardiol. 2020 Oct;147:74-87. doi: 10.1016/j.yjmcc.2020.08.008. Epub 2020 Aug 20. J Mol Cell Cardiol. 2020. PMID: 32827510 Free PMC article.
-
Improvement of outcome prediction of hospitalized patients with COVID-19 by a dual marker strategy using high-sensitive cardiac troponin I and copeptin.Clin Res Cardiol. 2022 Mar;111(3):343-354. doi: 10.1007/s00392-021-01970-4. Epub 2021 Nov 15. Clin Res Cardiol. 2022. PMID: 34782921 Free PMC article.
-
Cardiac injury is associated with mortality and critically ill pneumonia in COVID-19: A meta-analysis.Am J Emerg Med. 2021 Jun;44:352-357. doi: 10.1016/j.ajem.2020.04.052. Epub 2020 Apr 19. Am J Emerg Med. 2021. PMID: 32331955 Free PMC article.
-
Prognostic performance of troponin in COVID-19: A diagnostic meta-analysis and meta-regression.Int J Infect Dis. 2021 Apr;105:312-318. doi: 10.1016/j.ijid.2021.02.113. Epub 2021 Mar 2. Int J Infect Dis. 2021. PMID: 33667694 Free PMC article.
Cited by
-
The impact of COVID-19 on myocardial infarctions, strokes and out-of-hospital cardiopulmonary arrests: an observational retrospective study on time-sensitive disorders in the Friuli Venezia Giulia region (Italy).Int J Emerg Med. 2022 Dec 29;15(1):68. doi: 10.1186/s12245-022-00473-x. Int J Emerg Med. 2022. PMID: 36581807 Free PMC article.
-
Subclinical myocardial injury, coagulopathy, and inflammation in COVID-19: A meta-analysis of 41,013 hospitalized patients.Int J Cardiol Heart Vasc. 2022 Jun;40:100950. doi: 10.1016/j.ijcha.2021.100950. Epub 2022 Jan 4. Int J Cardiol Heart Vasc. 2022. PMID: 35005211 Free PMC article.
-
Fragmented QRS is a marker of mortality in patients with severe COVID-19: A retrospective observational study.Anatol J Cardiol. 2021 Nov;25(11):811-820. doi: 10.5152/AnatolJCardiol.2021.62. Anatol J Cardiol. 2021. PMID: 34734815 Free PMC article.
-
New-Onset Atrial Fibrillation in the Critically Ill COVID-19 Patients Hospitalized in the Intensive Care Unit.J Clin Med. 2023 Nov 8;12(22):6989. doi: 10.3390/jcm12226989. J Clin Med. 2023. PMID: 38002603 Free PMC article. Review.
-
Predictors of in-hospital mortality in critically ill patients with COVID-19: a large dual tertiary centre study.BMJ Open. 2022 Dec 1;12(12):e059358. doi: 10.1136/bmjopen-2021-059358. BMJ Open. 2022. PMID: 36456009 Free PMC article.
References
-
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395:497–506. - PMC - PubMed
-
- Xu J, Yang X, Yang L, Zou X, Wang Y, Wu Y, Zhou T, Yuan Y, Qi H, Fu S, Liu H, Xia J, Xu Z, Yu Y, Li R, Ouyang Y, Wang R, Ren L, Hu Y, Xu D, Zhao X, Yuan S, Zhang D, Shang Y. Clinical course and predictors of 60-day mortality in 239 critically ill patients with COVID-19: a multicenter retrospective study from Wuhan, China. Crit Care 2020;24:394. - PMC - PubMed
-
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin definition. JAMA 2012;307:2526–2533. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
