

Changes in Morphology of the Urethral Rhabdosphincter Postpartum
- PMID: 33620902
- PMCID: PMC7905706
- DOI: 10.1097/SPV.0000000000001007
Changes in Morphology of the Urethral Rhabdosphincter Postpartum
Abstract
Objective: The aim of the study was to determine the effect of pregnancy on urethral rhabdosphincter cross-sectional area (CSA) and any association of CSA to urinary symptoms.
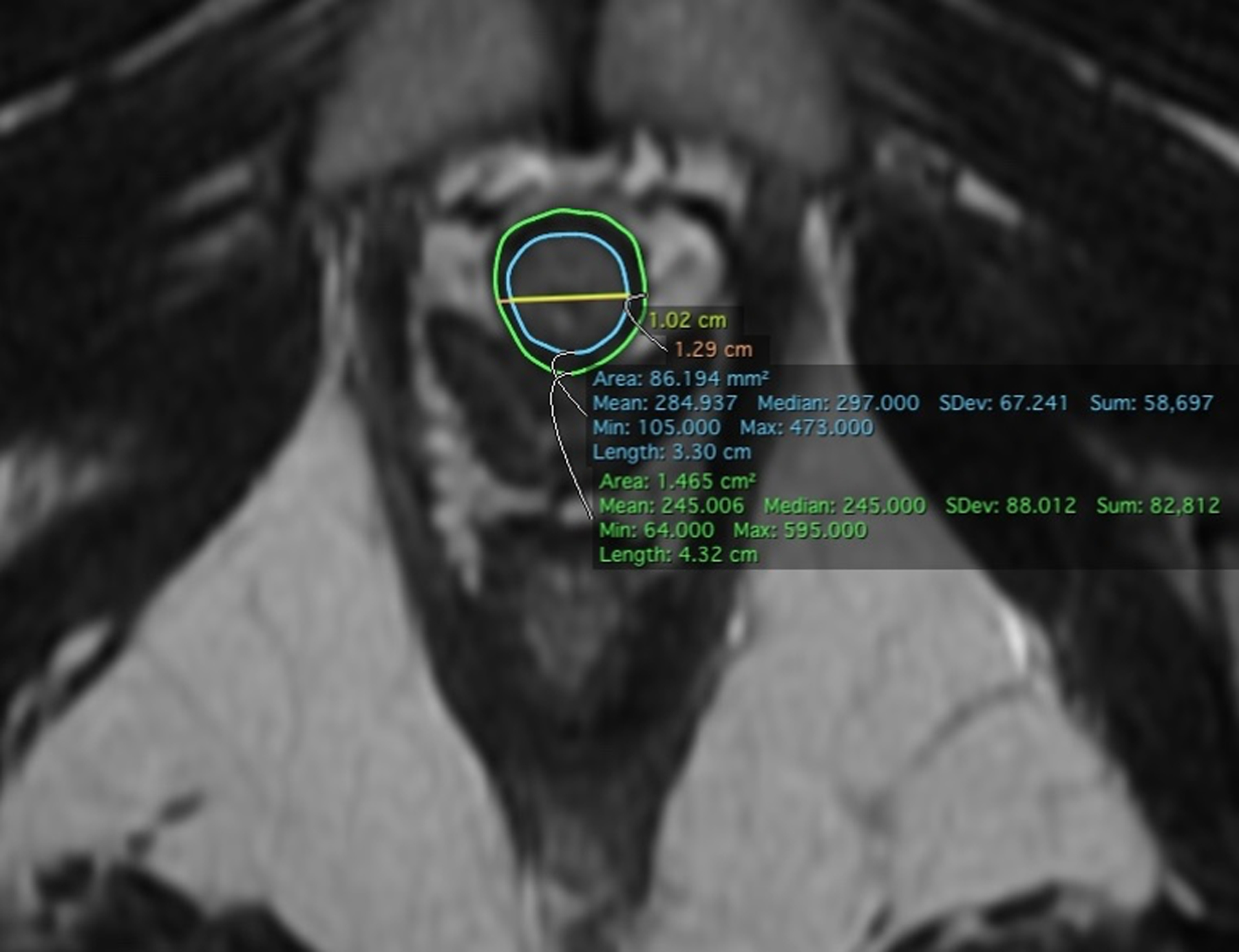
Methods: Nulliparous women planning pregnancy (N = 135) underwent standardized evaluations (symptom and quality of life [QOL] questionnaires, magnetic resonance imaging, ultrasonography, and neurophysiologic testing) between January 2008 and December 2013 (V1). The participants who became pregnant and gave birth underwent the same evaluations at 6 weeks (V2) and 6 months postpartum (V3). Participants who had magnetic resonance imaging data from both V1 and V3 were selected. We measured urethral rhabdosphincter CSA from high-resolution axial MRIs in a masked fashion. The mean CSA for each participant was calculated. The change from V1 to V3 was assessed.
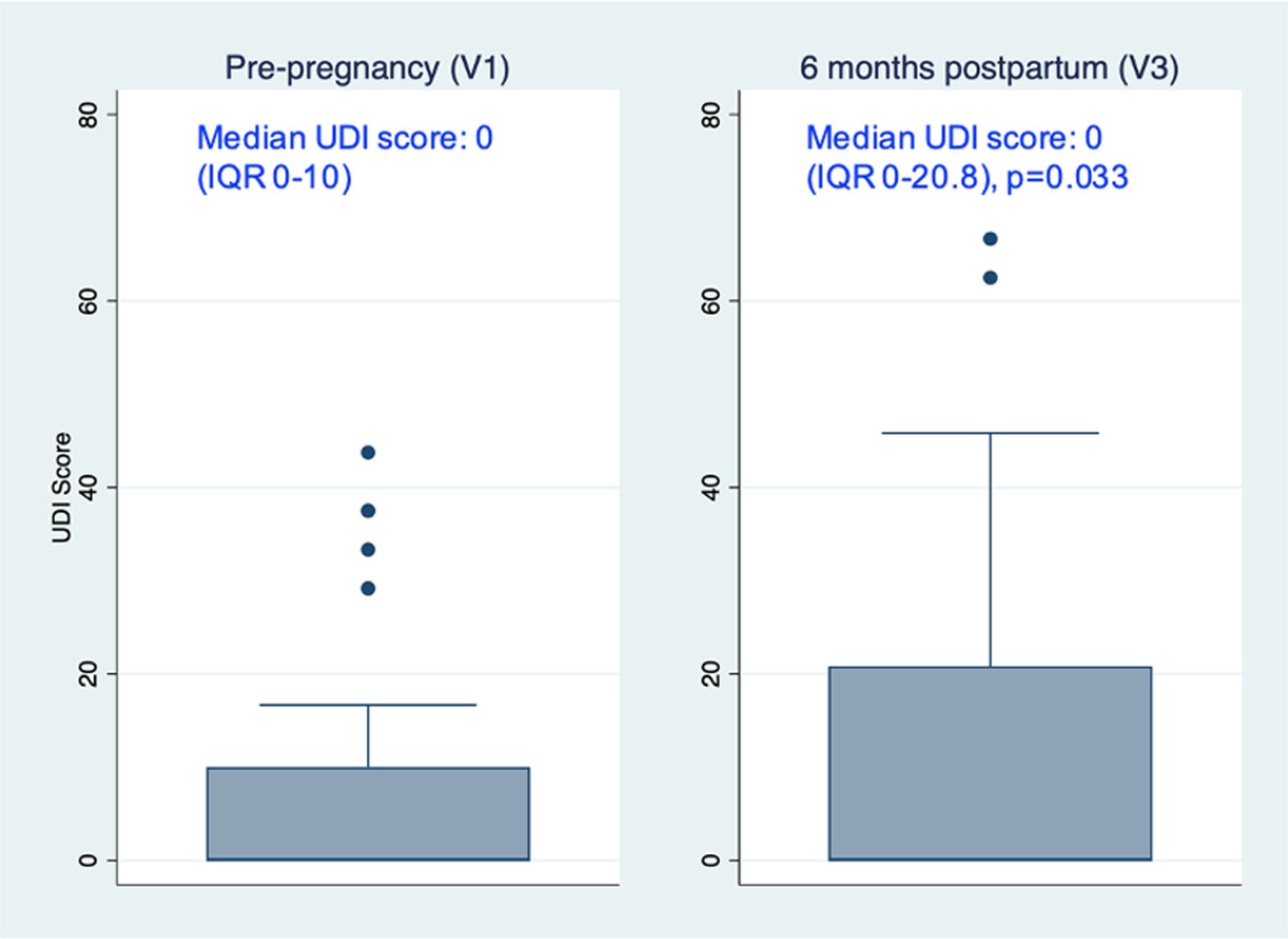
Results: Sixty-eight women were evaluated. There was a significant decrease of 0.05 cm2 (interquartile range, -0.03 to 0.16 cm2; P = 0.002) in the median sphincter CSA between V1 and V3. There was a significant increase in the median Urinary Distress Inventory (UDI) subscore of the Pelvic Floor Distress Inventory (PFDI) from V1 to V3 (median increase of 0 [IQR, 0 to 8.3]; P = 0.033), but this was not significantly correlated with the change in the urethral CSA (Spearman correlation, 0.199; P = 0.107). Increasing fetal weight was correlated with a decrease in CSA postpartum after vaginal birth (Spearman correlation, -0.340; P = 0.017).
Conclusions: There is a decrease in urethral rhabdosphincter CSA with worsening Urinary Distress Inventory scores from prepregnancy to postpartum, but these two do not correlate in this cohort with low symptom levels. Among women who give birth vaginally, decrease in rhabdosphincter CSA is correlated with increasing fetal weight, perhaps with ramifications to be seen later in life.
Copyright © 2021 American Urogynecologic Society. All rights reserved.
Figures


References
-
- Sangsawang B Risk factors for the development of stress urinary incontinence during pregnancy in primigravidae: a review of the literature. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2014;178:27–34. - PubMed
-
- Pizzoferrato A-C, Fauconnier A, Bader G, de Tayrac R, Fort J, Fritel X. Is prenatal urethral descent a risk factor for urinary incontinence during pregnancy and the postpartum period? International Urogynecology Journal. 2016;27(7):1003–1011. - PubMed
-
- van Veelen A, Schweitzer K, van der Vaart H. Ultrasound assessment of urethral support in women with stress urinary incontinence during and after first pregnancy. Obstet Gynecol. 2014;124(2 Pt 1):249–256. - PubMed
-
- Daly D, Clarke M, Begley C. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, type, and risk factors. International Urogynecology Journal. 2018;29(3):353–362. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
