

Comorbid illnesses are associated with altered adaptive immune responses to SARS-CoV-2
- PMID: 33621211
- PMCID: PMC8026190
- DOI: 10.1172/jci.insight.146242
Comorbid illnesses are associated with altered adaptive immune responses to SARS-CoV-2
Abstract
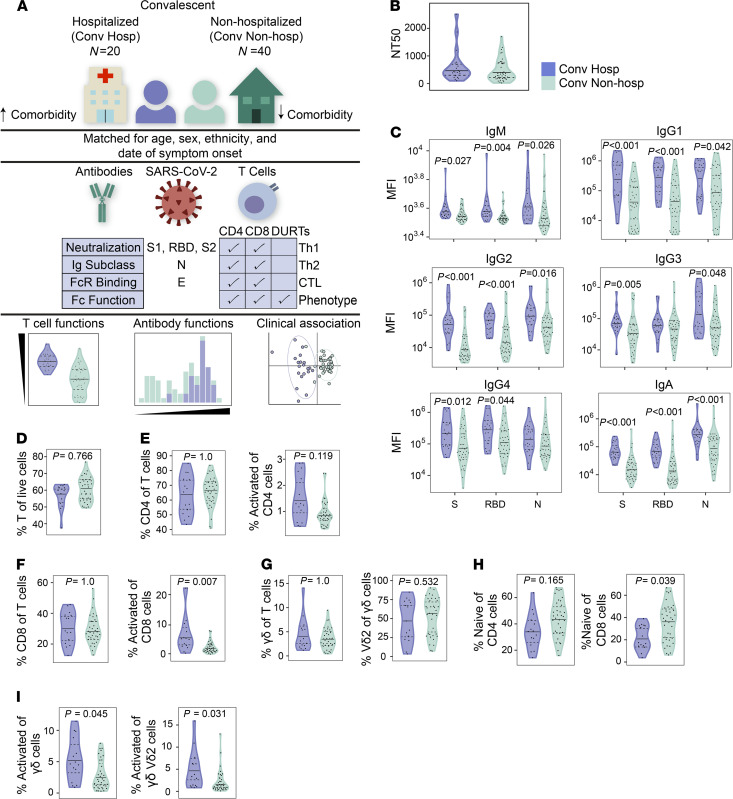
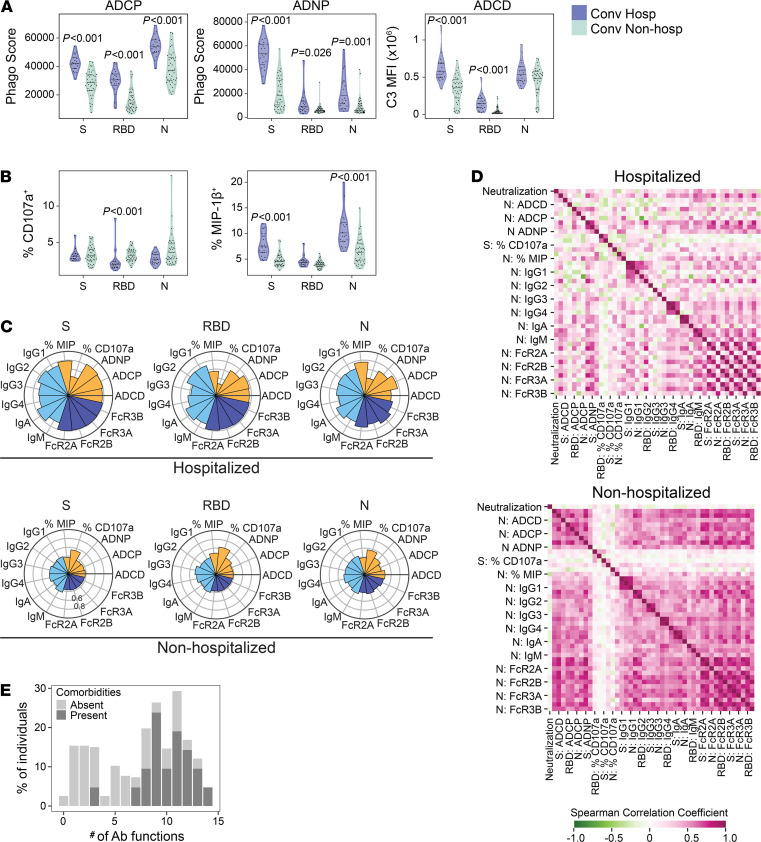
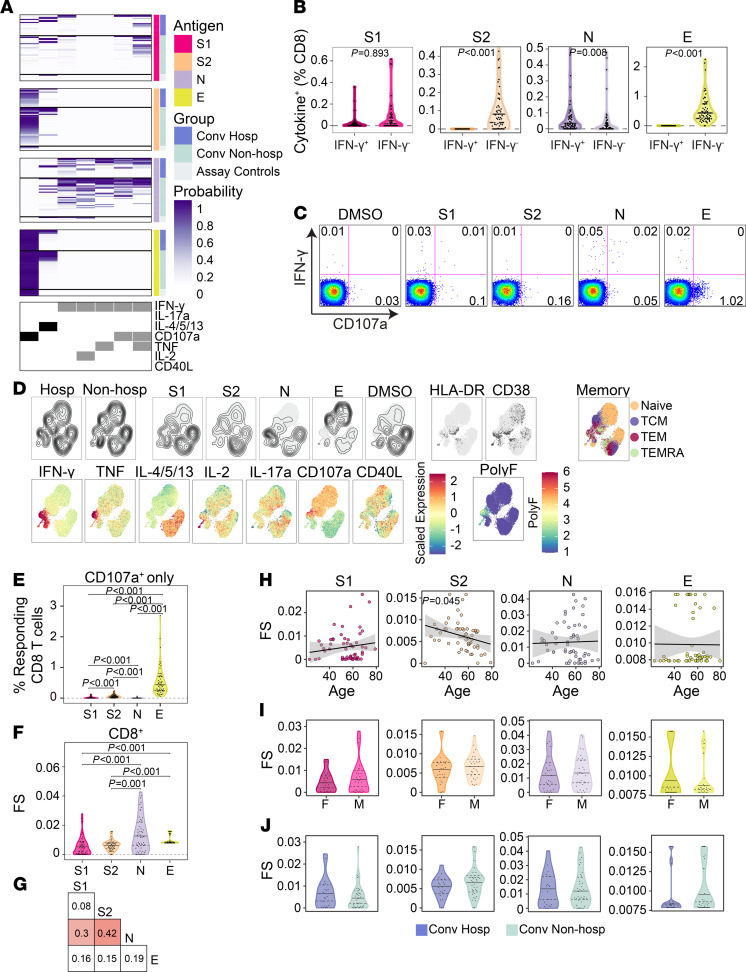
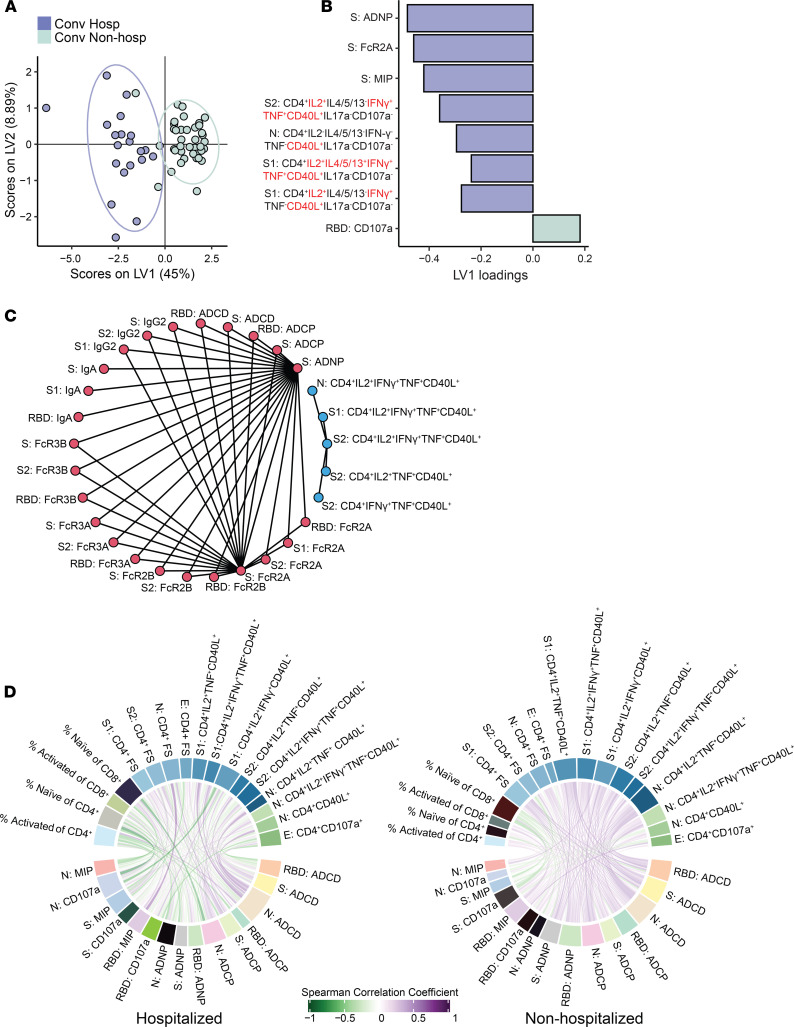
Comorbid medical illnesses, such as obesity and diabetes, are associated with more severe COVID-19, hospitalization, and death. However, the role of the immune system in mediating these clinical outcomes has not been determined. We used multiparameter flow cytometry and systems serology to comprehensively profile the functions of T cells and antibodies targeting spike, nucleocapsid, and envelope proteins in a convalescent cohort of COVID-19 subjects who were either hospitalized (n = 20) or not hospitalized (n = 40). To avoid confounding, subjects were matched by age, sex, ethnicity, and date of symptom onset. Surprisingly, we found that the magnitude and functional breadth of virus-specific CD4+ T cell and antibody responses were consistently higher among hospitalized subjects, particularly those with medical comorbidities. However, an integrated analysis identified more coordination between polyfunctional CD4+ T cells and antibodies targeting the S1 domain of spike among subjects who were not hospitalized. These data reveal a functionally diverse and coordinated response between T cells and antibodies targeting SARS-CoV-2, which is reduced in the presence of comorbid illnesses that are known risk factors for severe COVID-19.
Keywords: Adaptive immunity; Beta cells; COVID-19; Immunology; T cells.
Conflict of interest statement
Figures


Update of
-
T cell and antibody functional correlates of severe COVID-19.medRxiv [Preprint]. 2020 Nov 30:2020.11.25.20235150. doi: 10.1101/2020.11.25.20235150. medRxiv. 2020. Update in: JCI Insight. 2021 Mar 22;6(6):146242. doi: 10.1172/jci.insight.146242. PMID: 33269369 Free PMC article. Updated. Preprint.
Similar articles
-
T cell and antibody functional correlates of severe COVID-19.medRxiv [Preprint]. 2020 Nov 30:2020.11.25.20235150. doi: 10.1101/2020.11.25.20235150. medRxiv. 2020. Update in: JCI Insight. 2021 Mar 22;6(6):146242. doi: 10.1172/jci.insight.146242. PMID: 33269369 Free PMC article. Updated. Preprint.
-
Correlation of humoral immune responses to different SARS-CoV-2 antigens with virus neutralizing antibodies and symptomatic severity in a German COVID-19 cohort.Emerg Microbes Infect. 2021 Dec;10(1):774-781. doi: 10.1080/22221751.2021.1913973. Emerg Microbes Infect. 2021. PMID: 33830901 Free PMC article.
-
Sequential Analysis of Binding and Neutralizing Antibody in COVID-19 Convalescent Patients at 14 Months After SARS-CoV-2 Infection.Front Immunol. 2021 Nov 26;12:793953. doi: 10.3389/fimmu.2021.793953. eCollection 2021. Front Immunol. 2021. PMID: 34899762 Free PMC article.
-
SARS-CoV-2 Infection Severity Is Linked to Superior Humoral Immunity against the Spike.mBio. 2021 Jan 19;12(1):e02940-20. doi: 10.1128/mBio.02940-20. mBio. 2021. PMID: 33468695 Free PMC article.
-
Characterization of SARS-CoV-2-Specific Humoral and Cellular Immune Responses Induced by Inactivated COVID-19 Vaccines in a Real-World Setting.Front Immunol. 2021 Dec 22;12:802858. doi: 10.3389/fimmu.2021.802858. eCollection 2021. Front Immunol. 2021. PMID: 35003131 Free PMC article.
Cited by
-
Kinome and phosphoproteome reprogramming underlies the aberrant immune responses in critically ill COVID-19 patients.Clin Proteomics. 2024 Feb 22;21(1):13. doi: 10.1186/s12014-024-09457-w. Clin Proteomics. 2024. PMID: 38389037 Free PMC article.
-
Early cross-coronavirus reactive signatures of protective humoral immunity against COVID-19.bioRxiv [Preprint]. 2021 May 12:2021.05.11.443609. doi: 10.1101/2021.05.11.443609. bioRxiv. 2021. Update in: Sci Immunol. 2021 Oct 15;6(64):eabj2901. doi: 10.1126/sciimmunol.abj2901. PMID: 34013263 Free PMC article. Updated. Preprint.
-
Risk of extended viral shedding of Omicron BA.2 in Shanghai: Implications for vaccination strategy optimization.Chin Med J Pulm Crit Care Med. 2023 Dec 7;1(4):241-248. doi: 10.1016/j.pccm.2023.11.001. eCollection 2023 Dec. Chin Med J Pulm Crit Care Med. 2023. PMID: 39171280 Free PMC article.
-
Clinical outcomes in individuals hospitalized with SARS-CoV-2 Delta variant (B.1.617.2) who had been vaccinated with Covishield (ChAdOx1) and Covaxin (BBV-152).IJID Reg. 2022 Dec;5:104-110. doi: 10.1016/j.ijregi.2022.08.016. Epub 2022 Sep 5. IJID Reg. 2022. PMID: 36090517 Free PMC article.
-
The T cell immune response against SARS-CoV-2.Nat Immunol. 2022 Feb;23(2):186-193. doi: 10.1038/s41590-021-01122-w. Epub 2022 Feb 1. Nat Immunol. 2022. PMID: 35105982 Review.
References
-
- Virological. Novel 2019 Coronavirus Genome. https://virological.org/t/novel-2019-coronavirus-genome/319 Accessed February 19, 2021.
-
- Johns Hopkins University of Medicine. Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html Accessed February 19, 2021.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
