

Cost analysis of pediatric intensive care: a low-middle income country perspective
- PMID: 33622310
- PMCID: PMC7901186
- DOI: 10.1186/s12913-021-06166-0
Cost analysis of pediatric intensive care: a low-middle income country perspective
Abstract
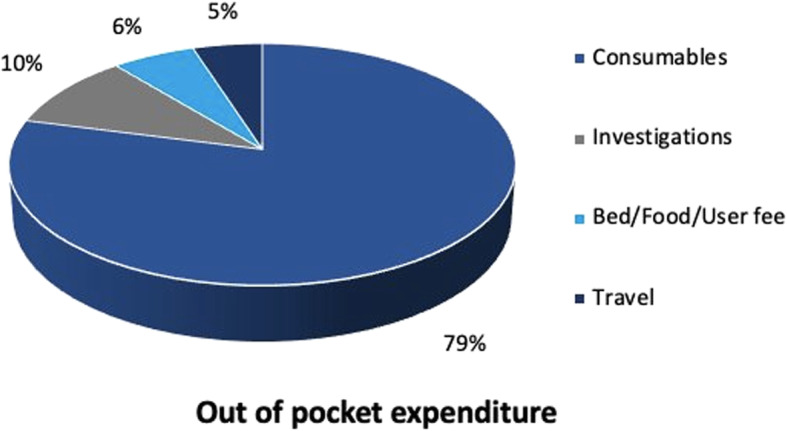
Background: Globally, Pediatric Intensive Care Unit (PICU) admissions are amongst the most expensive. In low middle-income countries, out of pocket expenditure (OOP) constitutes a major portion of the total expenditure. This makes it important to gain insights into the cost of pediatric intensive care. We undertook this study to calculate the health system cost and out of pocket expenditure incurred per patient during PICU stay.
Methods: Prospective study conducted in a state of the art tertiary level PICU of a teaching and referral hospital. Bottom-up micro costing methods were used to assess the health system cost. Annual data regarding hospital resources used for PICU care was collected from January to December 2018. Data regarding OOP was collected from 299 patients admitted from July 2017 to December 2018. The latter period was divided into four intervals, each of four and a half months duration and data was collected for 1 month in each interval. Per patient and per bed day costs for treatment were estimated both from health system and patient's perspective.
Results: The median (inter-quartile range, IQR) length of PICU stay was 5(3-8) days. Mean ± SD Pediatric Risk of Mortality Score (PRISM III) score of the study cohort was 22.23 ± 7.3. Of the total patients, 55.9% (167) were ventilated. Mean cost per patient treated was US$ 2078(₹ 144,566). Of this, health system cost and OOP expenditure per patient were US$ 1731 (₹ 120,425) and 352 (₹ 24,535) respectively. OOP expenditure of a ventilated child was twice that of a non- ventilated child.
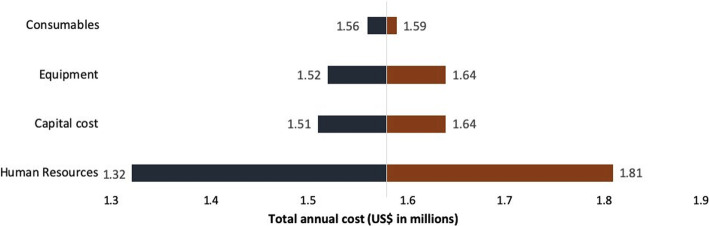
Conclusions: The fixed cost of PICU care was 3.8 times more than variable costs. Major portion of cost was borne by the hospital. Severe illness, longer ICU stay and ventilation were associated with increased costs. This study can be used to set the reimbursement package rates under Ayushman Bharat - Pradhan Mantri Jan Arogya Yojana (AB-PMJAY). Tertiary level intensive care in a public sector teaching hospital in India is far less expensive than developed countries.
Keywords: Cost analysis; Expenditure; Pediatric intensive care; Tertiary care.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
The Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) after four years of implementation - is it making an impact on quality of inpatient care and financial protection in India?BMC Health Serv Res. 2024 Aug 12;24(1):919. doi: 10.1186/s12913-024-11393-2. BMC Health Serv Res. 2024. PMID: 39135015 Free PMC article.
-
Out-of-Pocket Expenditure for Selected Surgeries in the Cardiology Department for Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY), Private Health Insurance, and Uninsured Patients in a Tertiary Care Teaching Hospital in Karnataka, India.Cureus. 2024 Jun 15;16(6):e62444. doi: 10.7759/cureus.62444. eCollection 2024 Jun. Cureus. 2024. PMID: 39015849 Free PMC article.
-
Out-of-Pocket Expenditure (OOPE) on Selected Surgeries in the Obstetrics and Gynaecology Department incurred by Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY), Private Health Insurance and Uninsured Patients in a Tertiary Care Teaching Hospital in Karnataka state of India.F1000Res. 2025 Jan 28;13:1511. doi: 10.12688/f1000research.157203.2. eCollection 2024. F1000Res. 2025. PMID: 39925993 Free PMC article.
-
Importance of Evidence-Based Health Insurance Reimbursement and Health Technology Assessment for Achieving Universal Health Coverage and Improved Access to Health in India.Value Health Reg Issues. 2021 May;24:24-30. doi: 10.1016/j.vhri.2020.04.007. Epub 2021 Jan 18. Value Health Reg Issues. 2021. PMID: 33476860 Review.
-
Averting catastrophic tuberculosis costs in an Indian state: integration of Ayushman Bharat Arogya Karnataka with National Tuberculosis Elimination Program.Lancet Reg Health Southeast Asia. 2023 Nov 23;22:100327. doi: 10.1016/j.lansea.2023.100327. eCollection 2024 Mar. Lancet Reg Health Southeast Asia. 2023. PMID: 38482155 Free PMC article. Review.
Cited by
-
Factors influencing the length of stay among patients admitted to a tertiary pediatric intensive care unit in Saudi Arabia.Front Pediatr. 2022 Dec 19;10:1093160. doi: 10.3389/fped.2022.1093160. eCollection 2022. Front Pediatr. 2022. PMID: 36601032 Free PMC article.
-
Challenges and Strategies in Pediatric Critical Care: Insights From Low-Resource Settings.Glob Pediatr Health. 2024 Sep 24;11:2333794X241285964. doi: 10.1177/2333794X241285964. eCollection 2024. Glob Pediatr Health. 2024. PMID: 39351100 Free PMC article. Review.
-
Impact of Benzodiazepines on Outcomes of Mechanically Ventilated Pediatric Intensive Care Patients: A Retrospective Cohort Study.Crit Care Explor. 2025 Apr 28;7(5):e1255. doi: 10.1097/CCE.0000000000001255. eCollection 2025 May 1. Crit Care Explor. 2025. PMID: 40293788 Free PMC article.
-
Disposition to pediatric intensive care unit post supraglottoplasty repair: a systematic review.J Otolaryngol Head Neck Surg. 2023 Apr 27;52(1):35. doi: 10.1186/s40463-023-00622-z. J Otolaryngol Head Neck Surg. 2023. PMID: 37106398 Free PMC article.
References
-
- Thompson DI. Reducing ICU costs with computerized tools. Healthc Financ Manage. 1995;49(6):66. - PubMed
-
- National Health Accounts | National Health Systems Resource Centre, MoHFW, Government of India [Internet]. [cited 2020 Nov 9]. Available from:http://nhsrcindia.org/category-detail/national-health-accounts/ODU=.
-
- Adamiak G. Methods for the economic evaluation of health care programmes, 3rd ed. J Epidemiol Community Health. 2006;60(9):822–823.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
