

Use and impact of high intensity treatments in patients with traumatic brain injury across Europe: a CENTER-TBI analysis
- PMID: 33622371
- PMCID: PMC7901510
- DOI: 10.1186/s13054-020-03370-y
Use and impact of high intensity treatments in patients with traumatic brain injury across Europe: a CENTER-TBI analysis
Abstract
Purpose: To study variation in, and clinical impact of high Therapy Intensity Level (TIL) treatments for elevated intracranial pressure (ICP) in patients with traumatic brain injury (TBI) across European Intensive Care Units (ICUs).
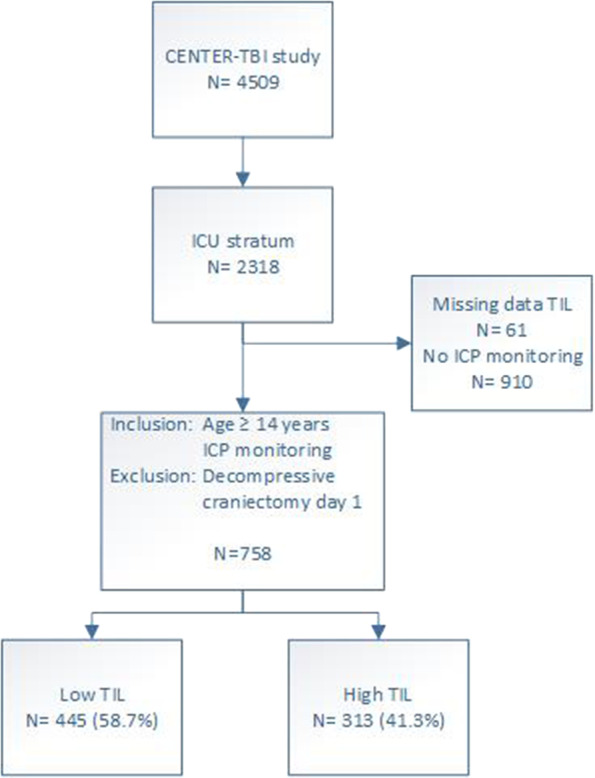
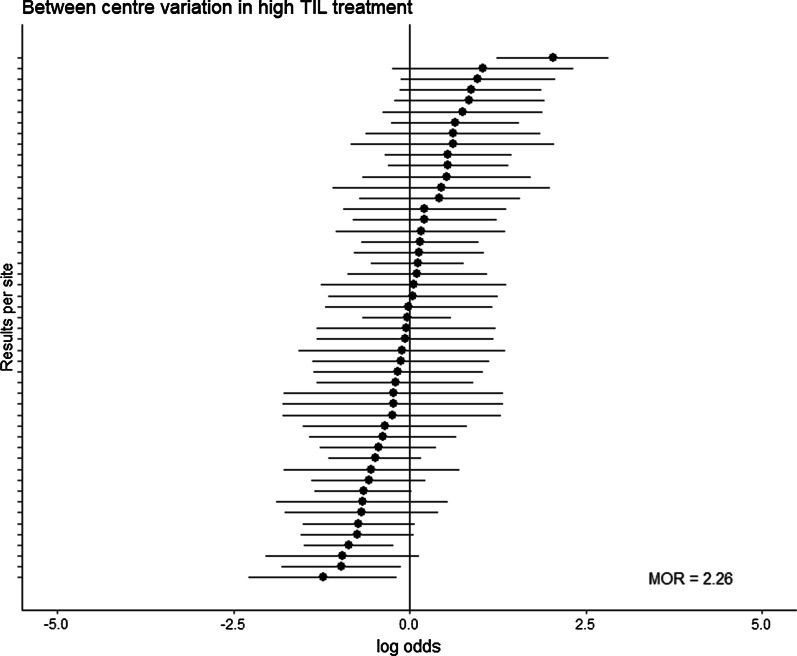
Methods: We studied high TIL treatments (metabolic suppression, hypothermia (< 35 °C), intensive hyperventilation (PaCO2 < 4 kPa), and secondary decompressive craniectomy) in patients receiving ICP monitoring in the ICU stratum of the CENTER-TBI study. A random effect logistic regression model was used to determine between-centre variation in their use. A propensity score-matched model was used to study the impact on outcome (6-months Glasgow Outcome Score-extended (GOSE)), whilst adjusting for case-mix severity, signs of brain herniation on imaging, and ICP.
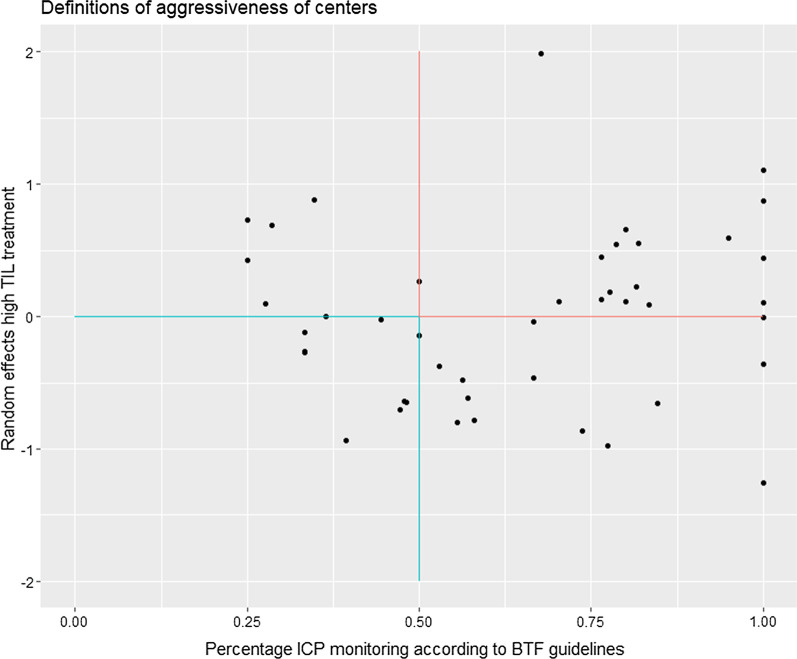
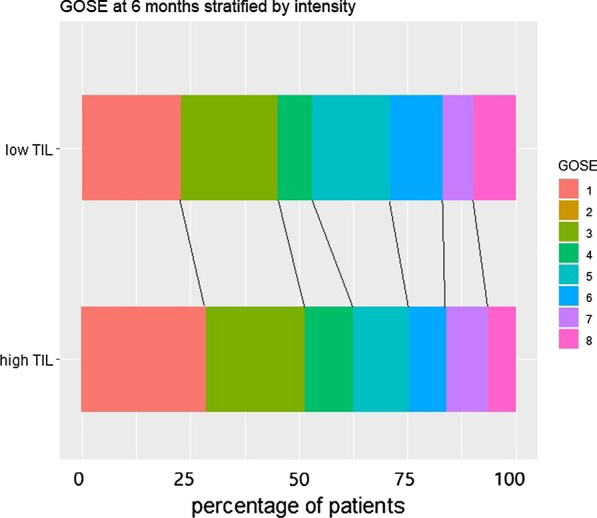
Results: 313 of 758 patients from 52 European centres (41%) received at least one high TIL treatment with significant variation between centres (median odds ratio = 2.26). Patients often transiently received high TIL therapies without escalation from lower tier treatments. 38% of patients with high TIL treatment had favourable outcomes (GOSE ≥ 5). The use of high TIL treatment was not significantly associated with worse outcome (285 matched pairs, OR 1.4, 95% CI [1.0-2.0]). However, a sensitivity analysis excluding high TIL treatments at day 1 or use of metabolic suppression at any day did reveal a statistically significant association with worse outcome.
Conclusion: Substantial between-centre variation in use of high TIL treatments for TBI was found and treatment escalation to higher TIL treatments were often not preceded by more conventional lower TIL treatments. The significant association between high TIL treatments after day 1 and worse outcomes may reflect aggressive use or unmeasured confounders or inappropriate escalation strategies.
Take home message: Substantial variation was found in the use of highly intensive ICP-lowering treatments across European ICUs and a stepwise escalation strategy from lower to higher intensity level therapy is often lacking. Further research is necessary to study the impact of high therapy intensity treatments.
Trial registration: The core study was registered with ClinicalTrials.gov, number NCT02210221, registered 08/06/2014, https://clinicaltrials.gov/ct2/show/NCT02210221?id=NCT02210221&draw=1&rank=1 and with Resource Identification Portal (RRID: SCR_015582).
Keywords: Barbiturates; Decompressive craniectomy; Hyperventilation; Hypothermia; Therapy intensity level; Traumatic brain injury.
Conflict of interest statement
AIRM declares consulting fees from PresSura Neuro, Integra Life Sciences, and NeuroTrauma Sciences. DKM reports grants from the UK National Institute for Health Research, during the conduct of the study; grants, personal fees, and non-financial support from GlaxoSmithKline; personal fees from Neurotrauma Sciences, Lantmaanen AB, Pressura, and Pfizer, outside of the submitted work. WP reports grants from the Netherlands Brain Foundation. ES reports personal fees from Springer, during the conduct of the study. All other authors declare no competing interests.
Figures
References
-
- Shore PM, Hand LL, Roy L, Trivedi P, Kochanek PM, Adelson PD. Reliability and validity of the pediatric intensity level of therapy (PILOT) scale: a measure of the use of intracranial pressure-directed therapies. Crit Care Med. 2006;34(7):1981–1987. doi: 10.1097/01.CCM.0000220765.22184.ED. - DOI - PubMed
-
- Zuercher P, Groen JL, Aries MJ, Steyerberg EW, Maas AI, Ercole A, Menon DK. Reliability and validity of the therapy intensity level scale: analysis of clinimetric properties of a novel approach to assess management of intracranial pressure in traumatic brain injury. J Neurotrauma. 2016;33(19):1768–1774. doi: 10.1089/neu.2015.4266. - DOI - PubMed
-
- Cnossen MC, Polinder S, Andriessen TM, van der Naalt J, Haitsma I, Horn J, Franschman G, Vos PE, Steyerberg EW, Lingsma H. Causes and consequences of treatment variation in moderate and severe traumatic brain injury: a multicenter study. Crit Care Med. 2017;45(4):660–669. doi: 10.1097/CCM.0000000000002263. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
