

Three-Year Outcomes of Implantable Collamer Lens Followed by Excimer Laser Enhancement ("Bioptics") in the Treatment of High Myopic Astigmatism
- PMID: 33623364
- PMCID: PMC7896759
- DOI: 10.2147/OPTH.S283888
Three-Year Outcomes of Implantable Collamer Lens Followed by Excimer Laser Enhancement ("Bioptics") in the Treatment of High Myopic Astigmatism
Abstract
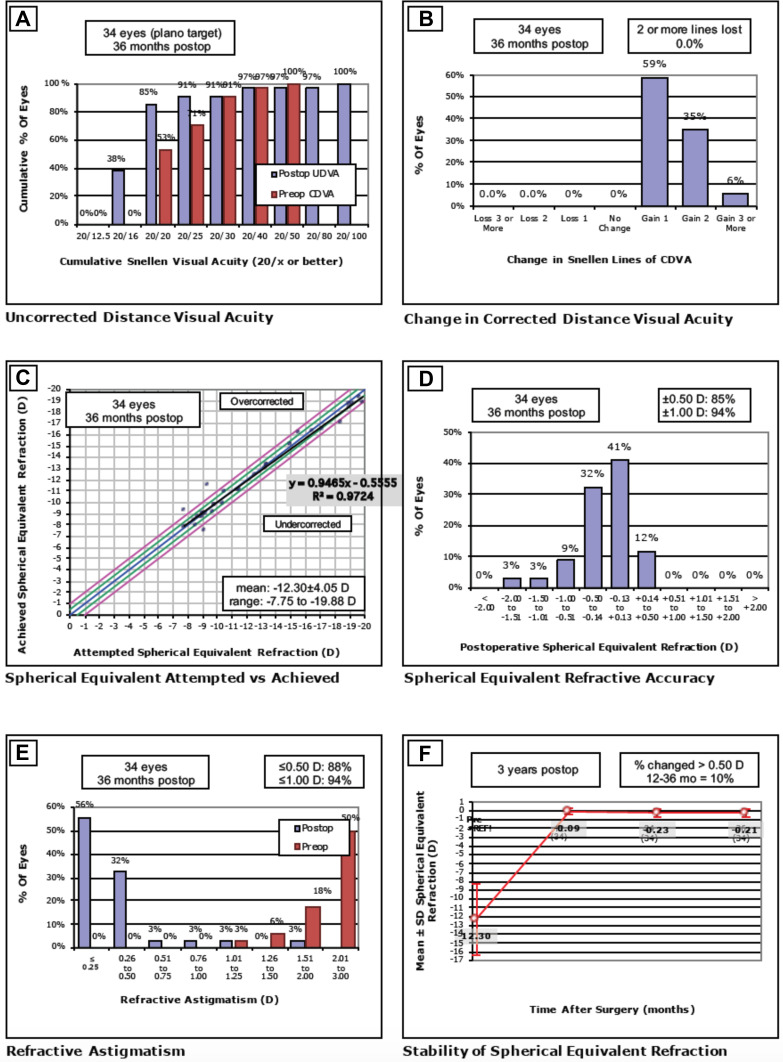
Purpose: Describe three-year outcomes of spherical implantable Collamer lens (ICL) followed by excimer laser enhancement (bioptics) in eyes with high myopic astigmatism.
Patients and methods: Retrospective case series of thirty-four cases that underwent bioptics enhancement at the Johns Hopkins Wilmer Eye Institute. All eyes had a preoperative sphere of -6.00 D or more with a cylinder of at least 2.00 D. Uncorrected and corrected distance visual acuity (UDVA and CDVA), manifest spherical equivalent refraction (MSE), ICL vault measurements and central corneal thickness (CCT) were collected. Endothelial cell counts (ECC), root mean square (RMS) of higher order aberrations (HOAs), adverse events and subsequent surgeries were also assessed.
Results: All patients had a minimum follow-up of 3 years. Preoperative UDVA was 2.29 ± 0.46 logMAR and improved to 0.03 ± 0.23 logMAR at 3 years (p<0.05). MSE was -12.30 ± 4.05 preoperatively and changed to -0.21 ± 0.46 at 3 years (p<0.05). The efficacy and safety indices were 1.28 ± 0.32 and 1.47 ± 0.27 at 3 years post-enhancement. HOA did not significantly change throughout the follow-up (p<0.05). Endothelial cell loss at 12 months was calculated at 5.7%. Two eyes required ICL exchange due to vault-related issues.
Conclusion: Bioptics offered excellent long-term safe, predictable, and efficient outcomes for high myopic astigmatism and can be considered an option if toric ICL is not available. Results confirm that wavefront-guided photoablation remains an excellent option to manage residual refractive error after phakic IOL.
Keywords: bioptics; enhancement; excimer laser; implantable collamer lens.
© 2021 Jabbour and Bower.
Conflict of interest statement
No conflicting relationships exist for any author.
Figures
Similar articles
-
Comparison of visual and refractive results of Toric Implantable Collamer Lens with bioptics for myopic astigmatism.Graefes Arch Clin Exp Ophthalmol. 2013 Mar;251(3):967-75. doi: 10.1007/s00417-012-2155-9. Epub 2012 Sep 23. Graefes Arch Clin Exp Ophthalmol. 2013. PMID: 23001585
-
Comparison of the toric implantable collamer lens and bioptics for myopic astigmatism.J Refract Surg. 2011 Feb;27(2):91-7. doi: 10.3928/1081597X-20100414-01. Epub 2010 Apr 15. J Refract Surg. 2011. PMID: 20438018
-
Visual Outcomes After Sequential Posterior Chamber Phakic IOL with Corneal Refractive Surgery (Bioptics) for the Treatment of Myopic Astigmatism.Clin Ophthalmol. 2020 Dec 9;14:4337-4346. doi: 10.2147/OPTH.S285140. eCollection 2020. Clin Ophthalmol. 2020. PMID: 33328722 Free PMC article.
-
One-year outcomes after intraocular collamer lens implantation in hyperopic astigmatism: a retrospective single-center study.Med Hypothesis Discov Innov Ophthalmol. 2024 Oct 14;13(3):112-120. doi: 10.51329/mehdiophthal1502. eCollection 2024 Fall. Med Hypothesis Discov Innov Ophthalmol. 2024. PMID: 39507812 Free PMC article.
-
Comparison of Collamer toric implantable [corrected] contact lens implantation and wavefront-guided laser in situ keratomileusis for high myopic astigmatism.J Cataract Refract Surg. 2008 Oct;34(10):1687-93. doi: 10.1016/j.jcrs.2008.06.030. J Cataract Refract Surg. 2008. PMID: 18812119
Cited by
-
Toric Implantable Collamer Lens for the Treatment of Myopic Astigmatism.Clin Ophthalmol. 2021 Jul 6;15:2893-2906. doi: 10.2147/OPTH.S321095. eCollection 2021. Clin Ophthalmol. 2021. PMID: 34262249 Free PMC article.
References
-
- Excimer laser photorefractive keratectomy (PRK) for myopia and astigmatism. American Academy of Ophthalmology. Ophthalmology. 1999;106(2):422–437. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
