

Antioxidative Capacity of Liver- and Adipose-Derived Mesenchymal Stem Cell-Conditioned Media and Their Applicability in Treatment of Type 2 Diabetic Rats
- PMID: 33623636
- PMCID: PMC7875634
- DOI: 10.1155/2021/8833467
Antioxidative Capacity of Liver- and Adipose-Derived Mesenchymal Stem Cell-Conditioned Media and Their Applicability in Treatment of Type 2 Diabetic Rats
Retraction in
-
Retracted: Antioxidative Capacity of Liver- and Adipose-Derived Mesenchymal Stem Cell-Conditioned Media and Their Applicability in Treatment of Type 2 Diabetic Rats.Oxid Med Cell Longev. 2024 Jan 9;2024:9854014. doi: 10.1155/2024/9854014. eCollection 2024. Oxid Med Cell Longev. 2024. PMID: 38234531 Free PMC article.
Abstract
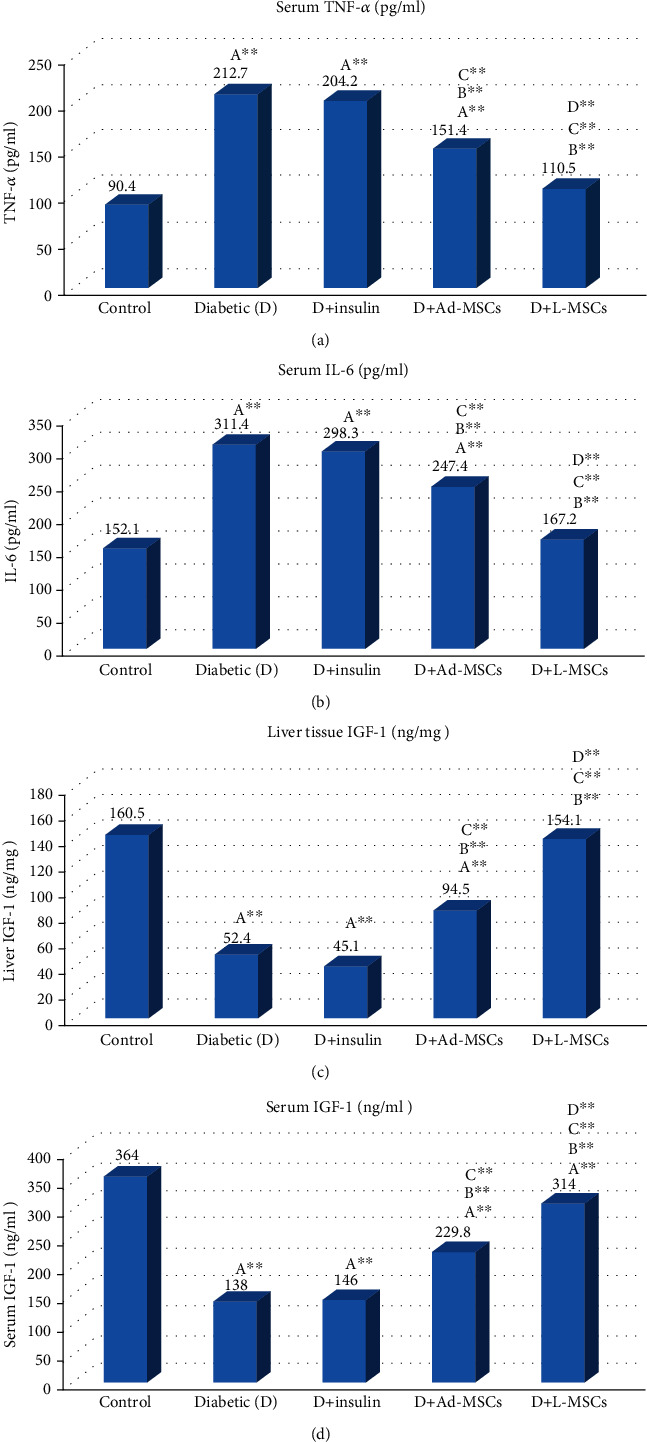
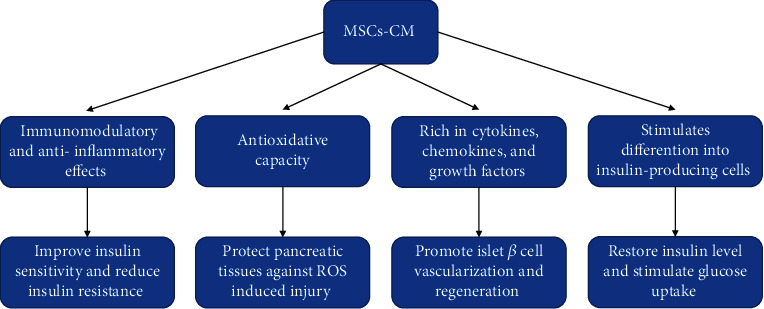
Type 2 diabetes mellitus (T2DM) is mainly characterized by insulin resistance and impaired insulin secretion, which cannot be reversed with existing therapeutic strategies. Using mesenchymal stem cells (MSCs), cell-based therapy has been demonstrated in displaying therapeutic effects in T2DM for their self-renewable, differentiation potential, and immunosuppressive properties and higher levels of angiogenic factors. Stem cell therapies are complicated and have a serious adverse effect including tumor formation and immunogenicity, while using mesenchymal stem cell-conditioned media (MSC-CM) significantly reduces stem cell risk, maintaining efficacy and showing significantly higher levels of growth factors, cytokines, and angiogenic factors that stimulate angiogenesis and promote fracture healing in diabetes. In the present study, we investigated the therapeutic potential of the liver and adipose MSC-CM in diabetic endothelial dysfunction compared with standard insulin therapy. Fifty adult male Sprague Dawley rats were divided equally into 5 groups as follows: control, diabetic, diabetic+insulin, diabetic+liver MSC-CM, and diabetic+adipose MSC-CM; all treatments continued for 4 weeks. Finally, we observed that liver MSC-CM therapy had the most apparent improvement in levels of blood glucose; HbA1c; AGEs; lipid panel (cholesterol, TG, LDL, HDL, and total lipids); renal function (urea, uric acid, creatinine, and total protein); liver function (AST, ALT, ALP, bilirubin, and albumin); CPK; C-peptide; HO-1; inflammatory markers including IL-6, TNF-α, and CRP; growth factors (liver and serum IGF-1); amylase; histopathological changes; pancreatic cell oxidative stress; and antioxidant markers (MDA, GSH, ROS, CAT, SOD, HO-1, and XO) toward the normal levels compared with insulin and adipose MSCs-CM. Moreover, both the liver and adipose MSC-CM relieved the hyperglycemic status by improving pancreatic islet β cell regeneration, promoting the conversion of alpha cells to beta cells, reducing insulin resistance, and protecting pancreatic tissues against oxidative stress-induced injury as well as possessing the ability to modulate immunity and angiogenesis. These results indicated that MSC-CM infusion has therapeutic effects in T2DM rats and may be a promising novel therapeutic target.
Copyright © 2021 Mohamed M. Elshemy et al.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
"2-(4-Fluorobenzamido)-4-methylthiazole-5-carboxylic acid" a novel thiazole compound, ameliorates insulin sensitivity and hyperlipidaemia in streptozotocin-induced diabetic rats: Plausible role of inflammatory and oxidative stress markers.Biomed Pharmacother. 2017 Nov;95:1232-1241. doi: 10.1016/j.biopha.2017.09.014. Epub 2017 Oct 6. Biomed Pharmacother. 2017. PMID: 28938514
-
Treatment with adipose tissue-derived mesenchymal stem cells exerts anti-diabetic effects, improves long-term complications, and attenuates inflammation in type 2 diabetic rats.Stem Cell Res Ther. 2019 Nov 20;10(1):333. doi: 10.1186/s13287-019-1474-8. Stem Cell Res Ther. 2019. PMID: 31747961 Free PMC article.
-
Antidiabetic effect of total flavonoids from Sanguis draxonis in type 2 diabetic rats.J Ethnopharmacol. 2013 Oct 7;149(3):729-36. doi: 10.1016/j.jep.2013.07.035. Epub 2013 Aug 7. J Ethnopharmacol. 2013. PMID: 23933499
-
Applicability of adipose-derived mesenchymal stem cells in treatment of patients with type 2 diabetes.Stem Cell Res Ther. 2019 Aug 28;10(1):274. doi: 10.1186/s13287-019-1362-2. Stem Cell Res Ther. 2019. PMID: 31455405 Free PMC article. Review.
-
Type 2 Diabetes Mellitus Induced Paracrine Effects on Breast Cancer Metastasis Through Extracellular Vesicles Derived from Human Mesenchymal Stem Cells.Stem Cells Dev. 2020 Nov 1;29(21):1382-1394. doi: 10.1089/scd.2020.0126. Epub 2020 Oct 5. Stem Cells Dev. 2020. PMID: 32900278
Cited by
-
Therapeutic effect of adipose-derived mesenchymal stem cells (AD-MSCs) compared to pirfenidone on corticosteroid resistance in a mouse model of acute exacerbation of idiopathic pulmonary fibrosis.Histol Histopathol. 2022 Nov;37(11):1065-1083. doi: 10.14670/HH-18-493. Epub 2022 Jul 11. Histol Histopathol. 2022. PMID: 35816024
-
Cell Therapies and Gene Therapy for Diabetes: Current Progress.Curr Diabetes Rev. 2025;21(8):e130524229899. doi: 10.2174/0115733998292392240425122326. Curr Diabetes Rev. 2025. PMID: 38747221 Review.
-
Melatonin Promotes the Therapeutic Effect of Mesenchymal Stem Cells on Type 2 Diabetes Mellitus by Regulating TGF-β Pathway.Front Cell Dev Biol. 2021 Oct 15;9:722365. doi: 10.3389/fcell.2021.722365. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34722505 Free PMC article.
-
Human Placental Mesenchymal Stem Cells Relieve Primary Sclerosing Cholangitis via Upregulation of TGR5 in Mdr2-/- Mice and Human Intrahepatic Cholangiocyte Organoid Models.Research (Wash D C). 2023 Aug 17;6:0207. doi: 10.34133/research.0207. eCollection 2023. Research (Wash D C). 2023. PMID: 37600495 Free PMC article.
-
Therapeutic effects of mesenchymal stem cell conditioned media on streptozotocin-induced diabetes in Wistar rats.Regen Ther. 2024 Nov 27;28:1-11. doi: 10.1016/j.reth.2024.11.004. eCollection 2025 Mar. Regen Ther. 2024. PMID: 39678398 Free PMC article.
References
-
- Aring A. M., Jones D. E., Falko J. M. Evaluation and prevention of diabetic neuropathy. American Family Physician. 2005;71(11):2123–2128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
