

Acute kidney injury pathology and pathophysiology: a retrospective review
- PMID: 33623675
- PMCID: PMC7886540
- DOI: 10.1093/ckj/sfaa142
Acute kidney injury pathology and pathophysiology: a retrospective review
Abstract
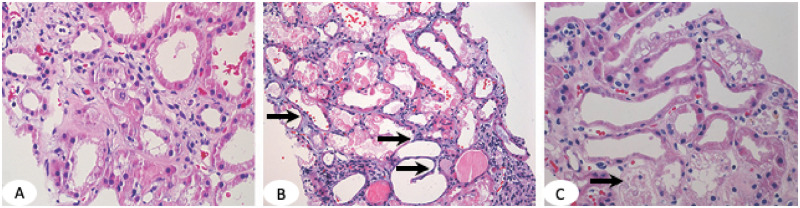
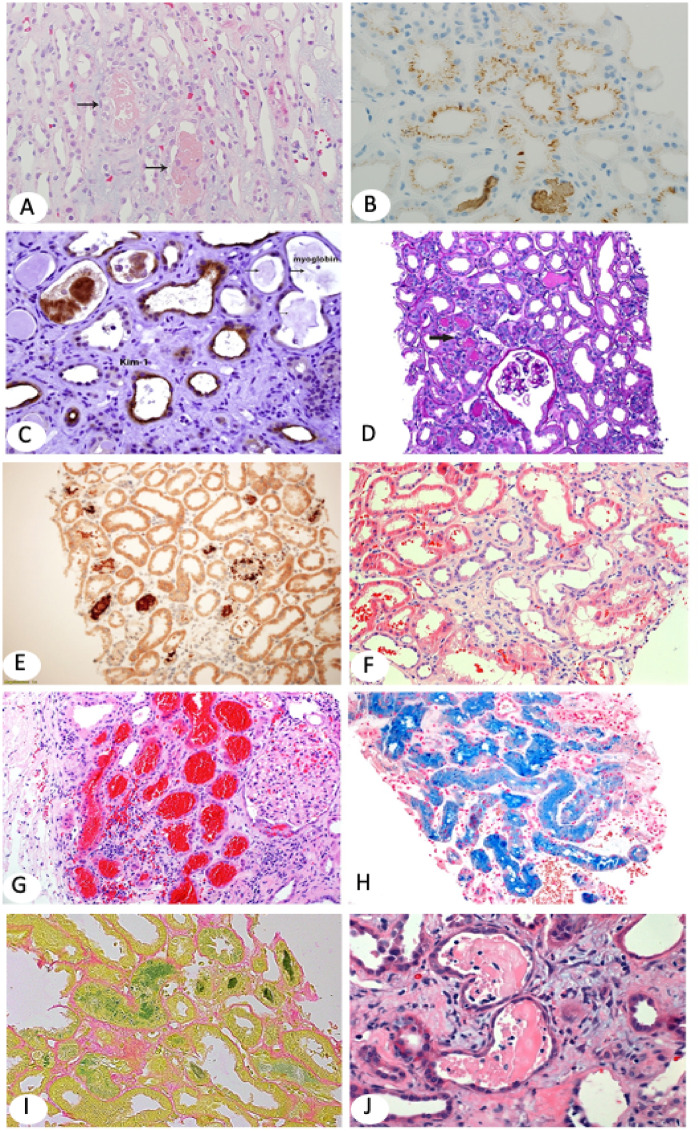
Acute kidney injury (AKI) is the clinical term used for decline or loss of renal function. It is associated with chronic kidney disease (CKD) and high morbidity and mortality. However, not all causes of AKI lead to severe consequences and some are reversible. The underlying pathology can be a guide for treatment and assessment of prognosis. The Kidney Disease: Improving Global Outcomes guidelines recommend that the cause of AKI should be identified if possible. Renal biopsy can distinguish specific AKI entities and assist in patient management. This review aims to show the pathology of AKI, including glomerular and tubular diseases.
Keywords: AKI; acute tubular necrosis; hemoglobinuria; multiple myeloma; pathology; pathophysiology; review; rhabdomyolysis.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Brun CC, Munck O. Lesions of the kidney in acute renal failure following shock. Lancet 1957; 269: 603–607 - PubMed
-
- Smith HM. The Kidney: Structure and Function in Health and Disease. 1st edn. Oxford: Oxford University Press, 1951
-
- Bellomo R, Kellum JA, Ronco C. Defining acute renal failure: physiological principles. Intensive Care Med 2004; 30: 33–37 - PubMed
-
- Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet 2019; 394: 1949–1964 - PubMed
-
- Kidney Disease: Improving Global Outcomes Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; 2: 1–138
Publication types
LinkOut - more resources
Full Text Sources
