

Net ultrafiltration rate and its impact on mortality in patients with acute kidney injury receiving continuous renal replacement therapy
- PMID: 33623680
- PMCID: PMC7886538
- DOI: 10.1093/ckj/sfz179
Net ultrafiltration rate and its impact on mortality in patients with acute kidney injury receiving continuous renal replacement therapy
Abstract
Background: Fluid overload, a critical consequence of acute kidney injury (AKI), is associated with worse outcomes. The optimal fluid removal rate per day during continuous renal replacement therapy (CRRT) is unknown. The purpose of this study is to evaluate the impact of the ultrafiltration rate on mortality in critically ill patients with AKI receiving CRRT.
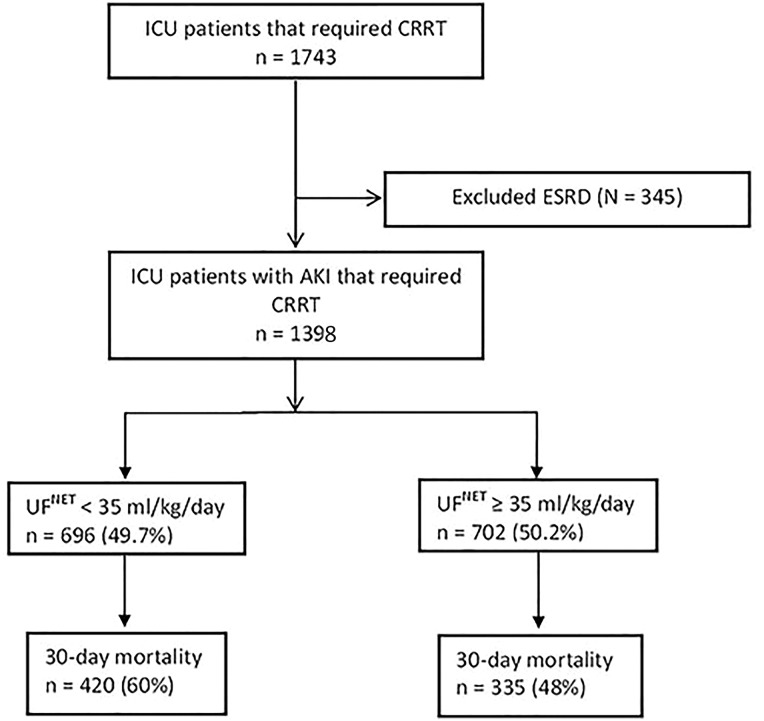
Methods: This was a retrospective cohort study where we reviewed 1398 patients with AKI who received CRRT between December 2006 and November 2015 at the Mayo Clinic, Rochester, MN, USA. The net ultrafiltration rate (UFNET) was categorized into low- and high-intensity groups (<35 and ≥35 mL/kg/day, respectively). The impact of different UFNET intensities on 30-day mortality was assessed using logistic regression after adjusting for age, sex, body mass index, fluid balance from intensive care unit (ICU) admission to CRRT initiation, Acute Physiologic Assessment and Chronic Health Evaluation III and sequential organ failure assessment scores, baseline serum creatinine, ICU day at CRRT initiation, Charlson comorbidity index, CRRT duration and need of mechanical ventilation.
Results: The mean ± SD age was 62 ± 15 years, and 827 (59%) were male. There were 696 patients (49.7%) in the low- and 702 (50.2%) in the high-intensity group. Thirty-day mortality was 755 (54%). There were 420 (60%) deaths in the low-, and 335 (48%) in the high-intensity group (P < 0.001). UFNET ≥35 mL/kg/day remained independently associated with lower 30-day mortality (adjusted odds ratio = 0.47, 95% confidence interval 0.37-0.59; P < 0.001) compared with <35 mL/kg/day.
Conclusions: More intensive fluid removal, UFNET ≥35 mL/kg/day, among AKI patients receiving CRRT is associated with lower mortality. Future prospective studies are required to confirm this finding.
Keywords: acute kidney injury; dose–response relationship; fluid overload; mortality; net ultrafiltration; renal replacement therapy.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Similar articles
-
Early net ultrafiltration thresholds and mortality in critically ill patients with septic acute kidney injury receiving continuous renal replacement therapy.Ren Fail. 2025 Dec;47(1):2511277. doi: 10.1080/0886022X.2025.2511277. Epub 2025 May 29. Ren Fail. 2025. PMID: 40437987 Free PMC article.
-
Net ultrafiltration intensity and mortality in critically ill patients with fluid overload.Crit Care. 2018 Sep 24;22(1):223. doi: 10.1186/s13054-018-2163-1. Crit Care. 2018. PMID: 30244678 Free PMC article.
-
[Effect of early initiation of continuous renal replacement therapy based on the KDIGO classification on the prognosis of critically ill patients with acute kidney injury].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016 Mar;28(3):246-51. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016. PMID: 29917340 Chinese.
-
Accelerated versus standard initiation of renal replacement therapy for critically ill patients with acute kidney injury: a systematic review and meta-analysis of RCT studies.Crit Care. 2021 Jan 5;25(1):5. doi: 10.1186/s13054-020-03434-z. Crit Care. 2021. PMID: 33402204 Free PMC article.
-
Fluid Overload and Precision Net Ultrafiltration in Critically Ill Patients.Cardiorenal Med. 2023;13(1):9-18. doi: 10.1159/000527390. Epub 2022 Oct 6. Cardiorenal Med. 2023. PMID: 36202071 Free PMC article. Review.
Cited by
-
Farewell from the CKJ Editor-in-Chief: key kidney topics from 2014 to 2021.Clin Kidney J. 2022 Mar 31;15(4):593-602. doi: 10.1093/ckj/sfac023. eCollection 2022 Apr. Clin Kidney J. 2022. PMID: 35371456 Free PMC article.
-
Early restrictive fluid balance is associated with lower hospital mortality independent of acute disease severity in critically ill patients on CRRT.Sci Rep. 2021 Sep 14;11(1):18216. doi: 10.1038/s41598-021-97888-y. Sci Rep. 2021. PMID: 34521957 Free PMC article.
-
Prediction of hemodynamic tolerance of intermittent hemodialysis in critically ill patients: a cohort study.Sci Rep. 2021 Dec 8;11(1):23610. doi: 10.1038/s41598-021-03110-4. Sci Rep. 2021. PMID: 34880359 Free PMC article.
-
Early net ultrafiltration thresholds and mortality in critically ill patients with septic acute kidney injury receiving continuous renal replacement therapy.Ren Fail. 2025 Dec;47(1):2511277. doi: 10.1080/0886022X.2025.2511277. Epub 2025 May 29. Ren Fail. 2025. PMID: 40437987 Free PMC article.
-
A Case Series: Continuous Kidney Replacement Therapy in Neonates With Low Body Weight.Front Pediatr. 2021 Nov 17;9:769220. doi: 10.3389/fped.2021.769220. eCollection 2021. Front Pediatr. 2021. PMID: 34869123 Free PMC article.
References
-
- Ostermann ME, Taube D, Morgan CJ et al.. Acute renal failure following cardiopulmonary bypass: a changing picture. Intensive Care Med 2000; 26: 565–571 - PubMed
LinkOut - more resources
Full Text Sources
Medical
