

Impact of a Whole-Room Atomizing Disinfection System on Healthcare Surface Contamination, Pathogen Transfer, and Labor Efficiency
- PMID: 33623925
- PMCID: PMC7892299
- DOI: 10.1097/CCE.0000000000000340
Impact of a Whole-Room Atomizing Disinfection System on Healthcare Surface Contamination, Pathogen Transfer, and Labor Efficiency
Abstract
Objectives: Healthcare surfaces contribute to nosocomial disease transmission. Studies show that despite standard guidelines and practices for cleaning and disinfection, secondary infection spread among healthcare workers and patients is common in ICUs. Manual terminal cleaning practices in healthcare are subject to highly variable results due to differences in training, compliance, and other inherent complexities. Standard cleaning practices combined with no-touch disinfecting technologies, however, may significantly lower nosocomial infection rates. The objective of this study was to evaluate the efficacy of a whole-room, no-touch disinfection intervention to reduce the concentration and cross-contamination of surface bacteria when used in tandem with manual cleaning protocols.
Design: Bacterial tracers were seeded onto hospital room surfaces to quantitatively evaluate the efficacy of manual terminal cleaning practices alone and in tandem with a no-touch, whole-room atomization system. Cross-contamination potentials and labor efficiency were also evaluated.
Subjects and intervention: Environmental service personnel cleaning efficacy was evaluated pre and post application of manual terminal cleaning protocols alone and in tandem with a whole-room atomization system with an United States Environmental Protection Agency-registered hospital-grade hypochlorous acid disinfectant.
Setting: The study was conducted in an unoccupied patient room at Banner University Medical Center in Tucson, AZ. The room was located in a newly constructed ICU suite.
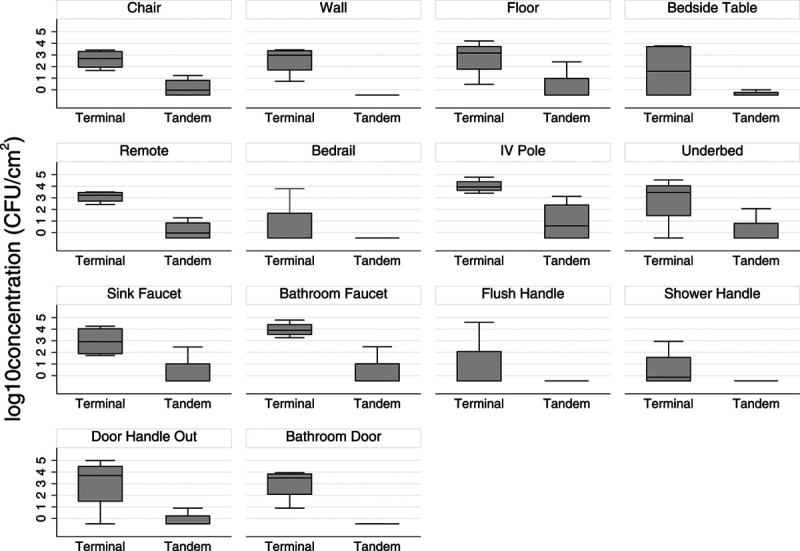
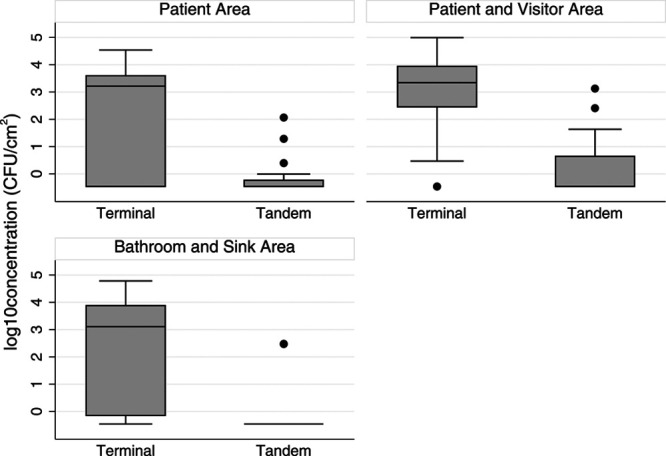
Measurements and main results: Manual terminal cleaning averaged a 2.4 log10 reduction in seeded bacterial counts compared with a 4.9 average and up to a 6 log10 reduction with tandem cleaning. Cross-contamination among surfaces following terminal cleaning alone was documented in 50% of the samples compared with 0% with tandem cleaning, with the latter achieving a 64% improvement in manual labor efficiency.
Conclusions: The use of whole-room atomized disinfection with terminal cleaning protocols lowered manual labor times, improved disinfection outcomes, and eliminated the transfer of bacterial pathogens in healthcare environments.
Keywords: bacterial tracer; cross-contamination; hospital fomites; hypochlorous acid; infection control; whole-room disinfection.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Reynolds has received research funds from Nevoa, Inc. The remaining authors have disclosed that they do not have any conflicts of interest.
Figures

Similar articles
-
Self-Disinfecting Copper Beds Sustain Terminal Cleaning and Disinfection Effects throughout Patient Care.Appl Environ Microbiol. 2019 Dec 13;86(1):e01886-19. doi: 10.1128/AEM.01886-19. Print 2019 Dec 13. Appl Environ Microbiol. 2019. PMID: 31704675 Free PMC article.
-
The impact of enhanced cleaning on bacterial contamination of the hospital environmental surfaces: a clinical trial in critical care unit in an Egyptian hospital.Antimicrob Resist Infect Control. 2024 Nov 19;13(1):138. doi: 10.1186/s13756-024-01489-z. Antimicrob Resist Infect Control. 2024. PMID: 39563364 Free PMC article. Clinical Trial.
-
Efficacy of pulsed-xenon ultraviolet light for disinfection of high-touch surfaces in an Ecuadorian hospital.BMC Infect Dis. 2019 Jul 3;19(1):575. doi: 10.1186/s12879-019-4200-3. BMC Infect Dis. 2019. PMID: 31269912 Free PMC article.
-
Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals.Antimicrob Resist Infect Control. 2016 Apr 11;5:10. doi: 10.1186/s13756-016-0111-x. eCollection 2016. Antimicrob Resist Infect Control. 2016. PMID: 27069623 Free PMC article. Review.
-
The role of the surface environment in healthcare-associated infections.Curr Opin Infect Dis. 2013 Aug;26(4):338-44. doi: 10.1097/QCO.0b013e3283630f04. Curr Opin Infect Dis. 2013. PMID: 23743816 Review.
Cited by
-
Experimental and CFD evaluation of ozone efficacy against coronavirus and enteric virus contamination on public transport surfaces.J Environ Chem Eng. 2021 Oct;9(5):106217. doi: 10.1016/j.jece.2021.106217. Epub 2021 Aug 17. J Environ Chem Eng. 2021. PMID: 34422551 Free PMC article.
-
Assessment of dry-fogged hydrogen peroxide as an "untact" room disinfection automation system for rapid terminal decontamination of a single isolation room in a healthcare institution.Antimicrob Resist Infect Control. 2025 Jul 26;14(1):92. doi: 10.1186/s13756-025-01613-7. Antimicrob Resist Infect Control. 2025. PMID: 40713741 Free PMC article.
-
Application of the defect management improvement mode under Joint Commission International standard to improve the instrument cleaning and disinfection effect and management quality in the central sterile supply department: a randomized trial.Ann Transl Med. 2022 Feb;10(3):137. doi: 10.21037/atm-21-6610. Ann Transl Med. 2022. PMID: 35284550 Free PMC article.
References
-
- Otter JA, Yezli S, Salkeld JA, et al. . Evidence that contaminated surfaces contribute to the transmission of hospital pathogens and an overview of strategies to address contaminated surfaces in hospital settings. Am J Infect Control. 2013; 41:S6–S11 - PubMed
-
- Weber DJ, Anderson D, Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis. 2013; 26:338–344 - PubMed
-
- Sehulster L, Chinn RY; CDC; HICPAC. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the healthcare infection control practices advisory committee (HICPAC). MMWR Recomm Rep. 2003; 52:1–42 - PubMed
-
- Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants. Arch Intern Med. 2006; 166:1945–1951 - PubMed
-
- Drees M, Snydman DR, Schmid CH, et al. . Prior environmental contamination increases the risk of acquisition of vancomycin-resistant enterococci. Clin Infect Dis. 2008; 46:678–685 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
