

Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers With the Risk of Hospitalization and Death in Hypertensive Patients With COVID-19
- PMID: 33624516
- PMCID: PMC8403305
- DOI: 10.1161/JAHA.120.018086
Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers With the Risk of Hospitalization and Death in Hypertensive Patients With COVID-19
Abstract
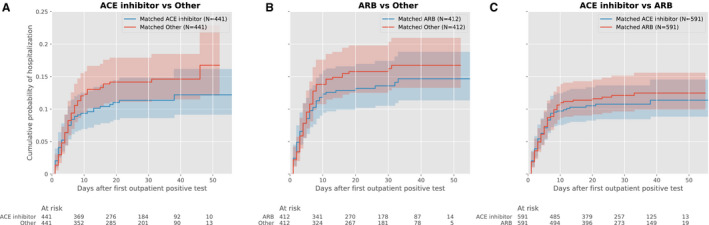
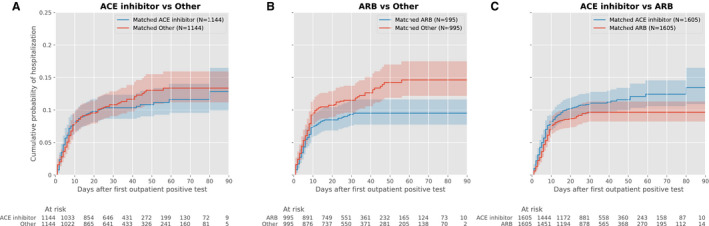
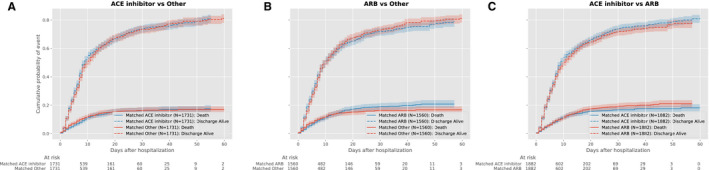
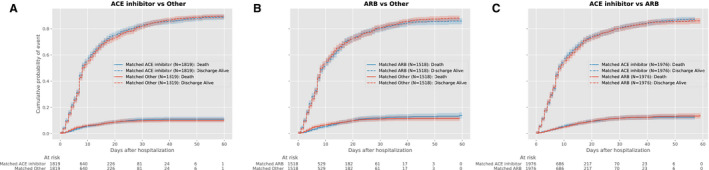
Background Despite its clinical significance, the risk of severe infection requiring hospitalization among outpatients with severe acute respiratory syndrome coronavirus 2 infection who receive angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) remains uncertain. Methods and Results In a propensity score-matched outpatient cohort (January-May 2020) of 2263 Medicare Advantage and commercially insured individuals with hypertension and a positive outpatient SARS-CoV-2, we determined the association of ACE inhibitors and ARBs with COVID-19 hospitalization. In a concurrent inpatient cohort of 7933 hospitalized with COVID-19, we tested their association with in-hospital mortality. The robustness of the observations was assessed in a contemporary cohort (May-August). In the outpatient study, neither ACE inhibitors (hazard ratio [HR], 0.77; 0.53-1.13, P=0.18) nor ARBs (HR, 0.88; 0.61-1.26, P=0.48) were associated with hospitalization risk. ACE inhibitors were associated with lower hospitalization risk in the older Medicare group (HR, 0.61; 0.41-0.93, P=0.02), but not the younger commercially insured group (HR, 2.14; 0.82-5.60, P=0.12; P-interaction 0.09). Neither ACE inhibitors nor ARBs were associated with lower hospitalization risk in either population in the validation cohort. In the primary inpatient study cohort, neither ACE inhibitors (HR, 0.97; 0.81-1.16; P=0.74) nor ARBs (HR, 1.15; 0.95-1.38, P=0.15) were associated with in-hospital mortality. These observations were consistent in the validation cohort. Conclusions ACE inhibitors and ARBs were not associated with COVID-19 hospitalization or mortality. Despite early evidence for a potential association between ACE inhibitors and severe COVID-19 prevention in older individuals, the inconsistency of this observation in recent data argues against a role for prophylaxis.
Keywords: COVID‐19; angiotensin receptor blockers; angiotensin‐converting enzyme inhibitors; hypertension.
Conflict of interest statement
Dr Krumholz was a recipient of a research grant, through Yale, from Medtronic and the US Food and Drug Administration to develop methods for postmarket surveillance of medical devices; was a recipient of a research grant with Medtronic and is the recipient of a research grant from Johnson & Johnson, through Yale University, to support clinical trial data sharing; was a recipient of a research agreement, through Yale University, from the Shenzhen Center for Health Information for work to advance intelligent disease prevention and health promotion; collaborates with the National Center for Cardiovascular Diseases in Beijing; receives payment from the Arnold & Porter Law Firm for work related to the Sanofi clopidogrel litigation, from the Martin/Baughman Law Firm for work related to the Cook Celect IVC filter litigation, and from the Siegfried and Jensen Law Firm for work related to Vioxx litigation; chairs a Cardiac Scientific Advisory Board for UnitedHealth; was a participant/participant representative of the IBM Watson Health Life Sciences Board; is a member of the Advisory Board for Element Science, the Advisory Board for Facebook, and the Physician Advisory Board for Aetna; and is a co‐founder of HugoHealth, a personal health information platform, and co‐founder of Refactor Health, an enterprise healthcare artificial intelligence–augmented data management company. He is also an advisor to FPrime. Drs Lin, Spatz, and Murugiah work under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures that are publicly reported. Dr Spatz receives support from the US Food and Drug Administration to support projects within the Yale‐Mayo Clinic Center of Excellence in Regulatory Science and Innovation (CERSI); the National Institute on Minority Health and Health Disparities (U54MD010711‐01) to study precision‐based approaches to diagnosing and preventing hypertension; and the National Institute of Biomedical Imaging and Bioengineering (R01EB028106‐01) to study a cuff‐less blood pressure device. Drs Clark, Ren, Vojta, and Mr Guo and Mr Truax are full‐time employees in Research & Development at UnitedHealth Group and own stock in the company. The remaining authors have no disclosures to report.
Figures
Update of
-
Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers with the Risk of Hospitalization and Death in Hypertensive Patients with Coronavirus Disease-19.medRxiv [Preprint]. 2020 May 19:2020.05.17.20104943. doi: 10.1101/2020.05.17.20104943. medRxiv. 2020. Update in: J Am Heart Assoc. 2021 Jul 6;10(13):e018086. doi: 10.1161/JAHA.120.018086. PMID: 32511481 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
