

Increased health care costs associated with new persistent opioid use after major surgery in opioid-naive patients
- PMID: 33624534
- PMCID: PMC8177715
- DOI: 10.18553/jmcp.2021.20507
Increased health care costs associated with new persistent opioid use after major surgery in opioid-naive patients
Abstract
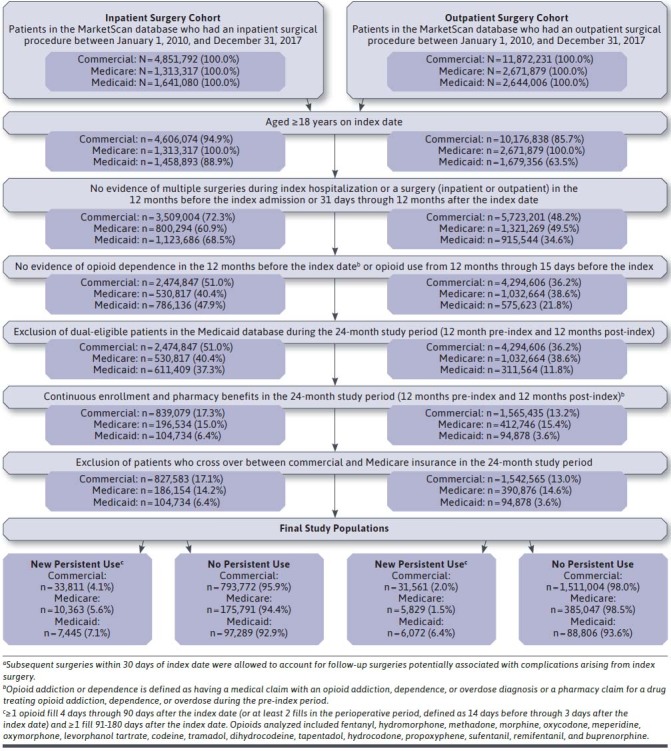
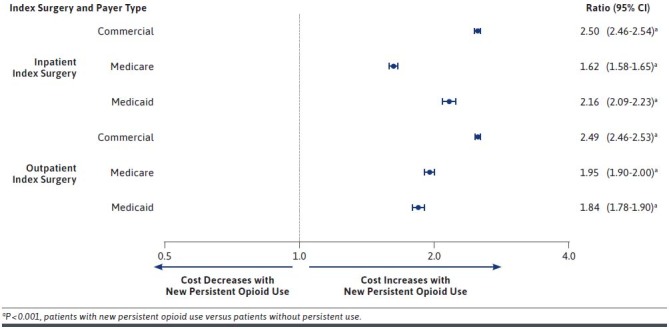
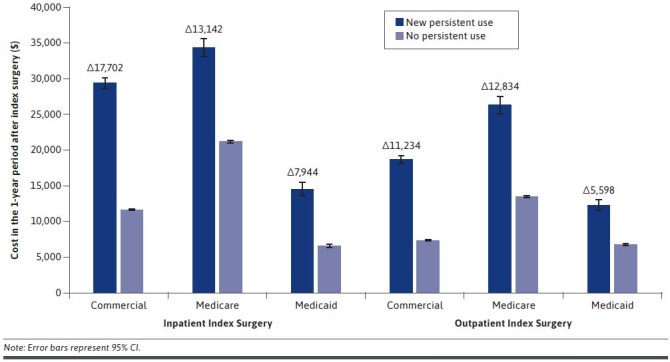
BACKGROUND: Opioid use after surgery is associated with increased health care utilization and costs. Although some studies show that surgical patients may later become persistent opioid users, data on the association between new persistent opioid use after surgery and health care utilization and costs are lacking. OBJECTIVE: To compare health care utilization and costs after major inpatient or METHODS: The IBM MarketScan Research databases were used to identify opioid-naive patients with major inpatient or outpatient surgeries and at least 1 year of continuous enrollment before and after this index surgery. Cohorts were stratified by new persistent opioid utilization status, setting of surgery (inpatient, outpatient), and payer (commercial, Medicare, Medicaid). Patients were considered new persistent opioid users if they had at least 1 opioid claim 4-90 days after index surgery and at least 1 opioid claim 91-180 days after index surgery. Patients with opioid prescription claims between 1 year and 15 days before their index event were excluded. Health care utilization and costs (excluding index surgery) were measured in the 1-year period after surgery. Predicted costs and cost ratios were estimated using multivariable log-linked gamma-family generalized linear models. RESULTS: In the inpatient cohorts, 827,583 commercial, 186,154 Medicare, and 104,734 Medicaid patients were included in the study, and the incidence of new persistent opioid use in these cohorts was 4.1%, 5.6%, and 7.1%, respectively. In the outpatient cohorts, 1,542,565 commercial, 390,876 Medicare, and 94,878 Medicaid patients were selected, with 2.0%, 1.5%, and 6.4% new persistent opioid use, respectively. Across all 3 payers in both surgical settings, patients with new persistent opioid use had a higher comorbidity burden and more use of concomitant medications in the baseline period. In the 1-year period after index surgery, patients with new persistent opioid use had more inpatient admissions, emergency department visits, and ambulance/paramedic service use than patients without persistent use, regardless of payer and setting. Patients with new persistent opioid use had approximately 5 times more opioid prescriptions and also had more nonopioid pharmacy claims than those without persistent use across all cohorts. After covariate adjustment, predicted 1-year total health care costs were significantly higher for patients with new persistent opioid use compared with those without persistent use for all comparisons (commercial inpatient: $29,499 vs. $11,798; Medicare inpatient: $34,455 vs. $21,313; Medicaid inpatient: $14,622 vs. $6,678; commercial outpatient: $18,751 vs. $7,517; Medicare outpatient ($26,411 vs. $13,577; Medicaid outpatient: $12,381 vs. $6,784; all P < 0.001). CONCLUSIONS: New persistent opioid use after major surgery in opioid-naive patients is associated with increased health care utilization and costs in the year after surgery across all surgical settings and payers. DISCLOSURES: Funding for this study was provided by Heron Therapeutics, which participated in analysis and interpretation of data, drafting, reviewing, and approving the publication. All authors contributed to the analysis and interpretation of the data and development of the publication and maintained control over the final content. England and Evans-Shields are employees of Heron Therapeutics. Kong, Lew, Zimmerman, and Henriques are employees of IBM Watson Health, which was compensated by Heron Therapeutics for conducting this research. Brummett is a paid consultant for Heron Therapeutics, Vertex Pharmaceuticals, and Alosa Health and provides expert testimony. He further reports receipt of research funding from MDHHS (Sub K Michigan Open), NIDA (Centralized Pain Opioid Non-Responsiveness R01 DA038261-05), NIH0DHHS-US-16 PAF 07628 (R01 NR017096-05), NIH-DHHS (P50 AR070600-05 CORT), NIH-DHHS-US (K23 DA038718-04), NIH-DHHS-US-16-PAF06270 (R01 HD088712-05), NIH-DHHS-US-17-PAF02680 (R01 DA042859-05), and UM Michigan Genomics Initiative and holds a patent for peripheral perineural dexmedetomidine. Sun reports funding from the National Institute on Drug Abuse (K08DA042314) as well as consulting fees from the Mission Lisa Foundation that are unrelated to this work.
Conflict of interest statement
Funding for this study was provided by Heron Therapeutics, which participated in analysis and interpretation of data, drafting, reviewing, and approving the publication. All authors contributed to the analysis and interpretation of the data and development of the publication and maintained control over the final content.
England and Evans-Shields are employees of Heron Therapeutics. Kong, Lew, Zimmerman, and Henriques are employees of IBM Watson Health, which was compensated by Heron Therapeutics for conducting this research. Brummett is a paid consultant for Heron Therapeutics, Vertex Pharmaceuticals, and Alosa Health and provides expert testimony. He further reports receipt of research funding from MDHHS (Sub K Michigan Open), NIDA (Centralized Pain Opioid Non-Responsiveness R01 DA038261-05), NIH0DHHS-US-16 PAF 07628 (R01 NR017096-05), NIH-DHHS (P50 AR070600-05 CORT), NIH-DHHS-US (K23 DA038718-04), NIH-DHHS-US-16-PAF06270 (R01 HD088712-05), NIH-DHHS-US-17-PAF02680 (R01 DA042859-05), and UM Michigan Genomics Initiative and holds a patent for peripheral perineural dexmedetomidine.
Sun reports funding from the National Institute on Drug Abuse (K08DA042314) as well as consulting fees from the Mission Lisa Foundation that are unrelated to this work.
Figures
References
-
- Centers for Disease Control and Prevention. 2019 annual surveillance report of drug-related risks and outcomes—United States surveillance special report. November 1, 2019. Accessed February 4, 2021. https://www.cdc.gov/drugoverdose/pdf/pubs/2019-cdc-drug-surveillance-rep...
-
- Leider HL, Dhaliwal J, Davis EJ, Kulakodlu M, Buikema AR. Healthcare costs and nonadherence among chronic opioid users. Am J Manag Care. 2011;17(1):32-40. - PubMed
-
- Kern DM, Zhou S, Chavoshi S, et al. . Treatment patterns, healthcare utilization, and costs of chronic opioid treatment for non-cancer pain in the United States. Am J Manag Care. 2015;21(3):e222-34. - PubMed
-
- Ghate SR, Haroutiunian S, Winslow R, McAdam-Marx C. Cost and comorbidities associated with opioid abuse in managed care and Medicaid patients in the United States: a comparison of two recently published studies. J Pain Palliat Care Pharmacother. 2010;24(3):251-58. - PubMed
-
- Rice JB, Kirson NY, Shei A, et al. . The economic burden of diagnosed opioid abuse among commercially insured individuals. Postgrad Med. 2014;126(4):53-58. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
