

Coronary Vasculature and Myocardial Structure in HIV: Physiologic Insights From the Renin-Angiotensin-Aldosterone System
- PMID: 33624807
- PMCID: PMC8864747
- DOI: 10.1210/clinem/dgab112
Coronary Vasculature and Myocardial Structure in HIV: Physiologic Insights From the Renin-Angiotensin-Aldosterone System
Abstract
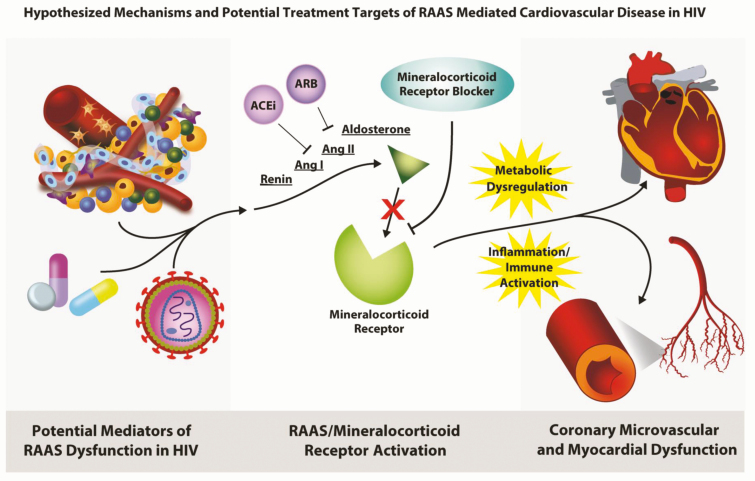
The landscape of HIV medicine dramatically changed with the advent of contemporary antiretroviral therapies, which has allowed persons with HIV (PWH) to achieve good virologic control, essentially eliminating HIV-related complications and increasing life expectancy. As PWH are living longer, noncommunicable diseases, such as cardiovascular disease (CVD), have become a leading cause of morbidity and mortality in PWH with rates that are 50% to 100% higher than in well-matched persons without HIV. In this review, we focus on disease of the coronary microvasculature and myocardium in HIV. We highlight a key hormonal system important to cardiovascular endocrinology, the renin-angiotensin-aldosterone system (RAAS), as a potential mediator of inflammatory driven-vascular and myocardial injury and consider RAAS blockade as a physiologically targeted strategy to reduce CVD in HIV.
Keywords: HIV; coronary flow reserve; eplerenone; myocardial dysfunction; renin-angiotensin-aldosterone system; sacubitril/valsartan.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- UNAIDS. Global HIV & AIDS statistics: 2020 fact sheet. 2020. https://www.unaids.org/en/resources/fact-sheet. Accessed October 14, 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
