

BACILLARY LAYER DETACHMENT BECAUSE OF MACULAR NEOVASCULARIZATION
- PMID: 33625111
- PMCID: PMC8371094
- DOI: 10.1097/IAE.0000000000003153
BACILLARY LAYER DETACHMENT BECAUSE OF MACULAR NEOVASCULARIZATION
Abstract
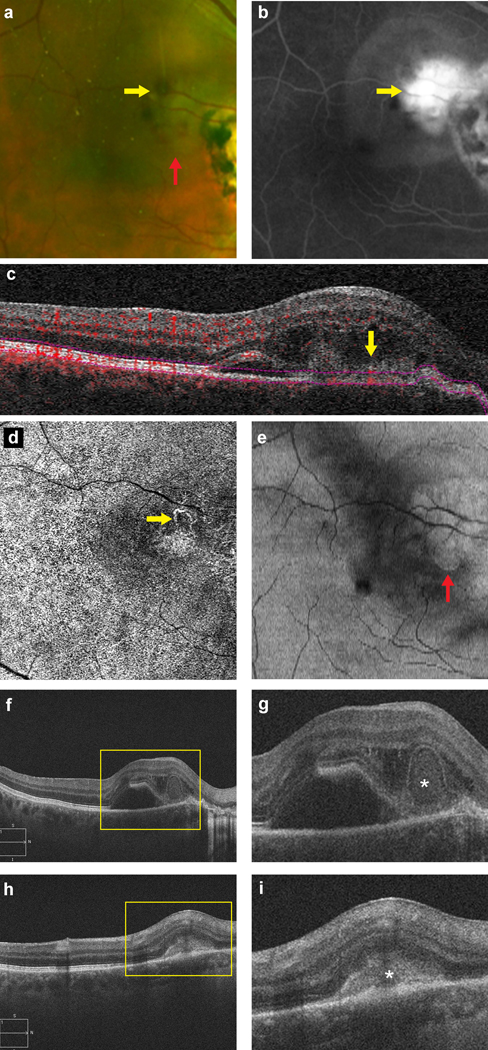
Purpose: To describe the clinical and multimodal imaging features of bacillary layer detachment (BD), and its response to intravitreal anti-vascular endothelial growth factor therapy, in eyes with macular neovascularization.
Methods: Retrospective, observational case series of 14 eyes (14 patients, 7 men) imaged with eyes (14 patients, 7 men) were imaged with spectral-domain optical coherence tomography, and either fluorescein angiography or optical coherence tomography angiography. Therapeutic response was monitored with serial imaging and best-corrected visual acuity assessments.
Results: The mean age was 75 ± 13 (range: 45-96) years, with mean follow-up duration of 27 ± 21 (range: 1-56) months. Neovascular age-related macular degeneration was found in 71% (10/14) eyes. Type 2 macular neovascularization lesions were associated with BD in all 14 eyes. Subretinal hemorrhage was noted in 79% (11/14) eyes. BD promptly resolved after intravitreal antivascular endothelial growth factor therapy in all eyes. The baseline best-corrected visual acuity improved from logarithm of the minimum angle of resolution 0.84 ± 0.32 (Snellen equivalent 20/138) to logarithm of the minimum angle of resolution 0.48 ± 0.31 (Snellen equivalent 20/60) at the last follow-up, with treatment of the macular neovascularization.
Conclusion: Type 2 macular neovascularization and subretinal hemorrhage are associated with BDs, which may be due to a rapid influx of exudative fluid into the potential space between the external limiting membrane and ellipsoid zone. Intravitreal antivascular endothelial growth factor therapy results in rapid resolution of BDs and visual improvement in most eyes.
Figures



Comment in
-
Reply.Retina. 2022 Jan 1;42(1):e1-e3. doi: 10.1097/IAE.0000000000003240. Retina. 2022. PMID: 34173360 Free PMC article.
-
Correspondence.Retina. 2022 Jan 1;42(1):e1. doi: 10.1097/IAE.0000000000003239. Retina. 2022. PMID: 34173363 No abstract available.
References
-
- Cuenca N, Ortuño-Lizarán I, Pinilla I. Cellular Characterization of OCT and Outer Retinal Bands Using Specific Immunohistochemistry Markers and Clinical Implications. Ophthalmology. 2018;125(3):407–422. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
