

Multidisciplinary Recommendations Regarding Post-Vaccine Adenopathy and Radiologic Imaging: Radiology Scientific Expert Panel
- PMID: 33625298
- PMCID: PMC7909071
- DOI: 10.1148/radiol.2021210436
Multidisciplinary Recommendations Regarding Post-Vaccine Adenopathy and Radiologic Imaging: Radiology Scientific Expert Panel
Abstract
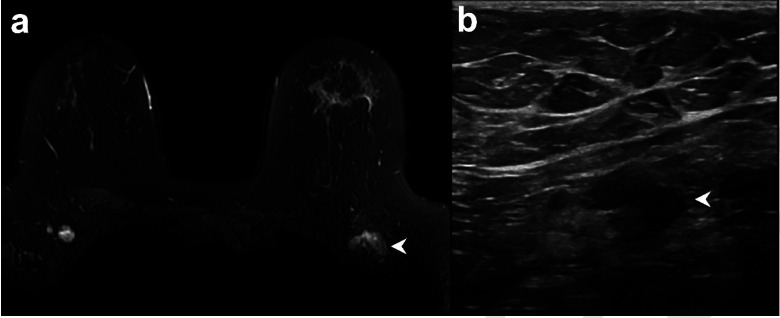
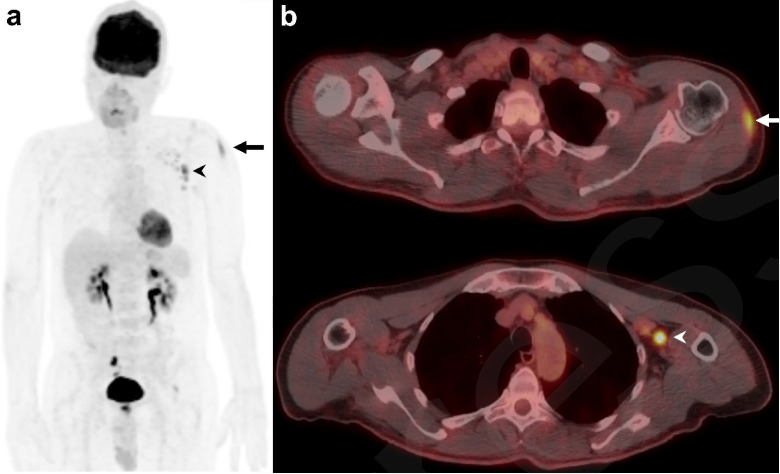
Vaccination-associated adenopathy is a frequent imaging finding after administration of COVID-19 vaccines that may lead to a diagnostic conundrum in patients with manifest or suspected cancer, in whom it may be indistinguishable from malignant nodal involvement. To help the medical community address this concern in the absence of studies and evidence-based guidelines, this special report offers recommendations developed by a multidisciplinary panel of experts from three of the leading tertiary care cancer centers in the United States. According to these recommendations, some routine imaging examinations, such as those for screening, should be scheduled before or at least 6 weeks after the final vaccination dose to allow for any reactive adenopathy to resolve. However, there should be no delay of other clinically indicated imaging (eg, for acute symptoms, short-interval treatment monitoring, urgent treatment planning or complications) due to prior vaccination. The vaccine should be administered on the side contralateral to the primary or suspected cancer, and both doses should be administered in the same arm. Vaccination information-date(s) administered, injection site(s), laterality, and type of vaccine-should be included in every preimaging patient questionnaire, and this information should be made readily available to interpreting radiologists. Clear and effective communication between patients, radiologists, referring physician teams, and the general public should be considered of the highest priority when managing adenopathy in the setting of COVID-19 vaccination.
© RSNA, 2021.
Figures
Comment in
-
COVID-19 Vaccination-Related Lymphadenopathy: What To Be Aware Of.Radiol Imaging Cancer. 2021 May;3(3):e210038. doi: 10.1148/rycan.2021210038. Radiol Imaging Cancer. 2021. PMID: 33874733 Free PMC article. No abstract available.
References
-
- Worldometers.info COVID-19 . https://www.worldometers.info/coronavirus/worldwide-graphs/. Accessed February 15, 2021.
-
- Frey SE, Couch RB, Tacket CO, et al. Clinical responses to undiluted and diluted smallpox vaccine. N Engl J Med 2002;346(17):1265–1274. doi:10.1056/NEJMoa020534. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
