

Screening for Atrial Fibrillation in the Older Population: A Randomized Clinical Trial
- PMID: 33625468
- PMCID: PMC7905702
- DOI: 10.1001/jamacardio.2021.0038
Screening for Atrial Fibrillation in the Older Population: A Randomized Clinical Trial
Abstract
Importance: Atrial fibrillation (AF) is a major cause of preventable strokes. Screening asymptomatic individuals for AF may increase anticoagulant use for stroke prevention.
Objective: To evaluate 2 home-based AF screening interventions.
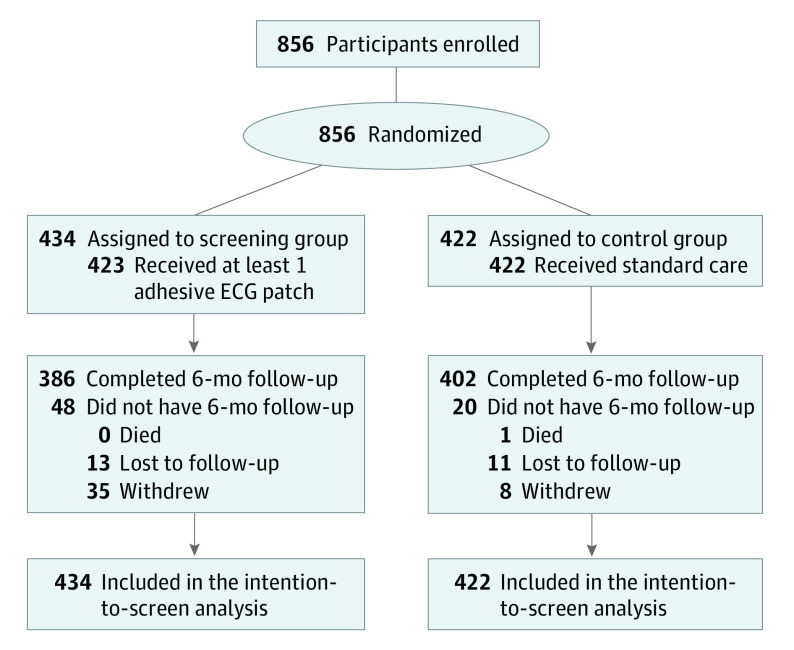
Design, setting, and participants: This multicenter randomized clinical trial recruited individuals from primary care practices aged 75 years or older with hypertension and without known AF. From April 5, 2015, to March 26, 2019, 856 participants were enrolled from 48 practices.
Interventions: The control group received standard care (routine clinical follow-up plus a pulse check and heart auscultation at baseline and 6 months). The screening group received a 2-week continuous electrocardiographic (cECG) patch monitor to wear at baseline and at 3 months, in addition to standard care. The screening group also received automated home blood pressure (BP) machines with oscillometric AF screening capability to use twice-daily during the cECG monitoring periods.
Main outcomes and measures: With intention-to-screen analysis, the primary outcome was AF detected by cECG monitoring or clinically within 6 months. Secondary outcomes included anticoagulant use, device adherence, and AF detection by BP monitors.
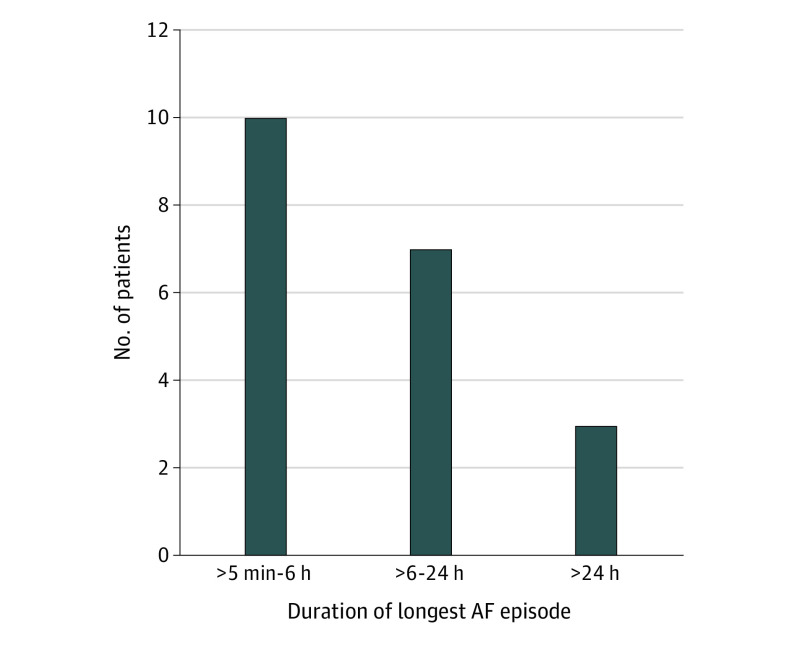
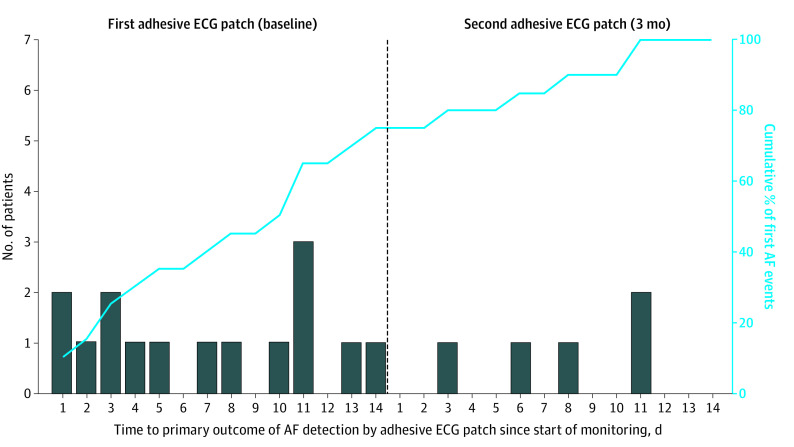
Results: Of the 856 participants, 487 were women (56.9%); mean (SD) age was 80.0 (4.0) years. Median cECG wear time was 27.4 of 28 days (interquartile range [IQR], 18.4-28.0 days). In the primary analysis, AF was detected in 23 of 434 participants (5.3%) in the screening group vs 2 of 422 (0.5%) in the control group (relative risk, 11.2; 95% CI, 2.7-47.1; P = .001; absolute difference, 4.8%; 95% CI, 2.6%-7.0%; P < .001; number needed to screen, 21). Of those with cECG-detected AF, median total time spent in AF was 6.3 hours (IQR, 4.2-14.0 hours; range 1.3 hours-28 days), and median duration of the longest AF episode was 5.7 hours (IQR, 2.9-12.9 hours). Anticoagulation was initiated in 15 of 20 patients (75.0%) with cECG-detected AF. By 6 months, anticoagulant therapy had been prescribed for 18 of 434 participants (4.1%) in the screening group vs 4 of 422 (0.9%) in the control group (relative risk, 4.4; 95% CI, 1.5-12.8; P = .007; absolute difference, 3.2%; 95% CI, 1.1%-5.3%; P = .003). Twice-daily AF screening using the home BP monitor had a sensitivity of 35.0% (95% CI, 15.4%-59.2%), specificity of 81.0% (95% CI, 76.7%-84.8%), positive predictive value of 8.9% (95% CI, 4.9%-15.5%), and negative predictive value of 95.9% (95% CI, 94.5%-97.0%). Adverse skin reactions requiring premature discontinuation of cECG monitoring occurred in 5 of 434 participants (1.2%).
Conclusions and relevance: In this randomized clinical trial, among older community-dwelling individuals with hypertension, AF screening with a wearable cECG monitor was well tolerated, increased AF detection 10-fold, and prompted initiation of anticoagulant therapy in most cases. Compared with continuous ECG, intermittent oscillometric screening with a BP monitor was an inferior strategy for detecting paroxysmal AF. Large trials with hard clinical outcomes are now needed to evaluate the potential benefits and harms of AF screening.
Trial registration: ClinicalTrials.gov Identifier: NCT02392754.
Conflict of interest statement
Figures
Comment in
-
Screening the Older Population for Atrial Fibrillation-Have We Moved the Needle Forward?JAMA Cardiol. 2021 May 1;6(5):495-496. doi: 10.1001/jamacardio.2021.0052. JAMA Cardiol. 2021. PMID: 33625482 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
