

Assessment of Outcomes Associated With the Use of Newly Approved Oncology Drugs in Medicare Beneficiaries
- PMID: 33625507
- PMCID: PMC7905499
- DOI: 10.1001/jamanetworkopen.2021.0030
Assessment of Outcomes Associated With the Use of Newly Approved Oncology Drugs in Medicare Beneficiaries
Abstract
Importance: A lack of generalizability of pivotal cancer clinical trial data to treatment of older adults with Medicare could affect therapeutic decision-making in clinical practice.
Objective: To evaluate the differences in survival, duration of therapy, and treatment patterns between clinical trial patients and older adults with Medicare receiving cancer drugs for metastatic solid cancers in usual practice.
Design, setting, and participants: This retrospective cohort study, performed from May 1, 2018, to August 30, 2020, used the linked Surveillance, Epidemiology, and End Results (SEER) program and Medicare database to examine sequential US Food and Drug Administration (FDA)-approved cancer drug indications (2008-2013) for locally advanced or metastatic solid tumors to assess whether pivotal trials reflect the outcomes of Medicare patients with cancer treated in usual practice.
Exposures: Treatment with FDA-approved cancer drugs for metastatic solid cancers in pivotal clinical trials and in the SEER-Medicare database.
Main outcomes and measures: Overall survival, duration of treatment, and dose reductions among trial participants and treated Medicare patients.
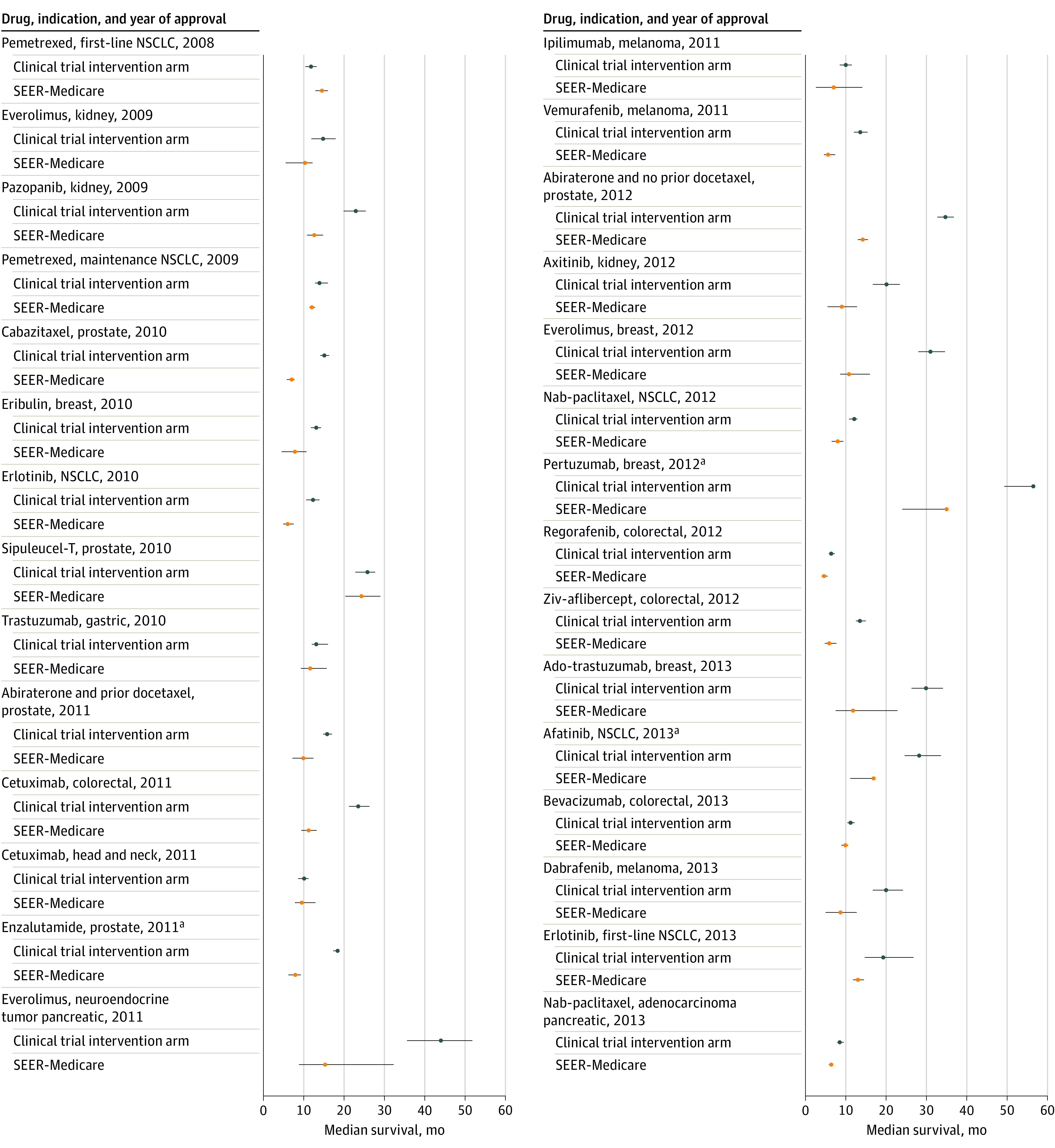
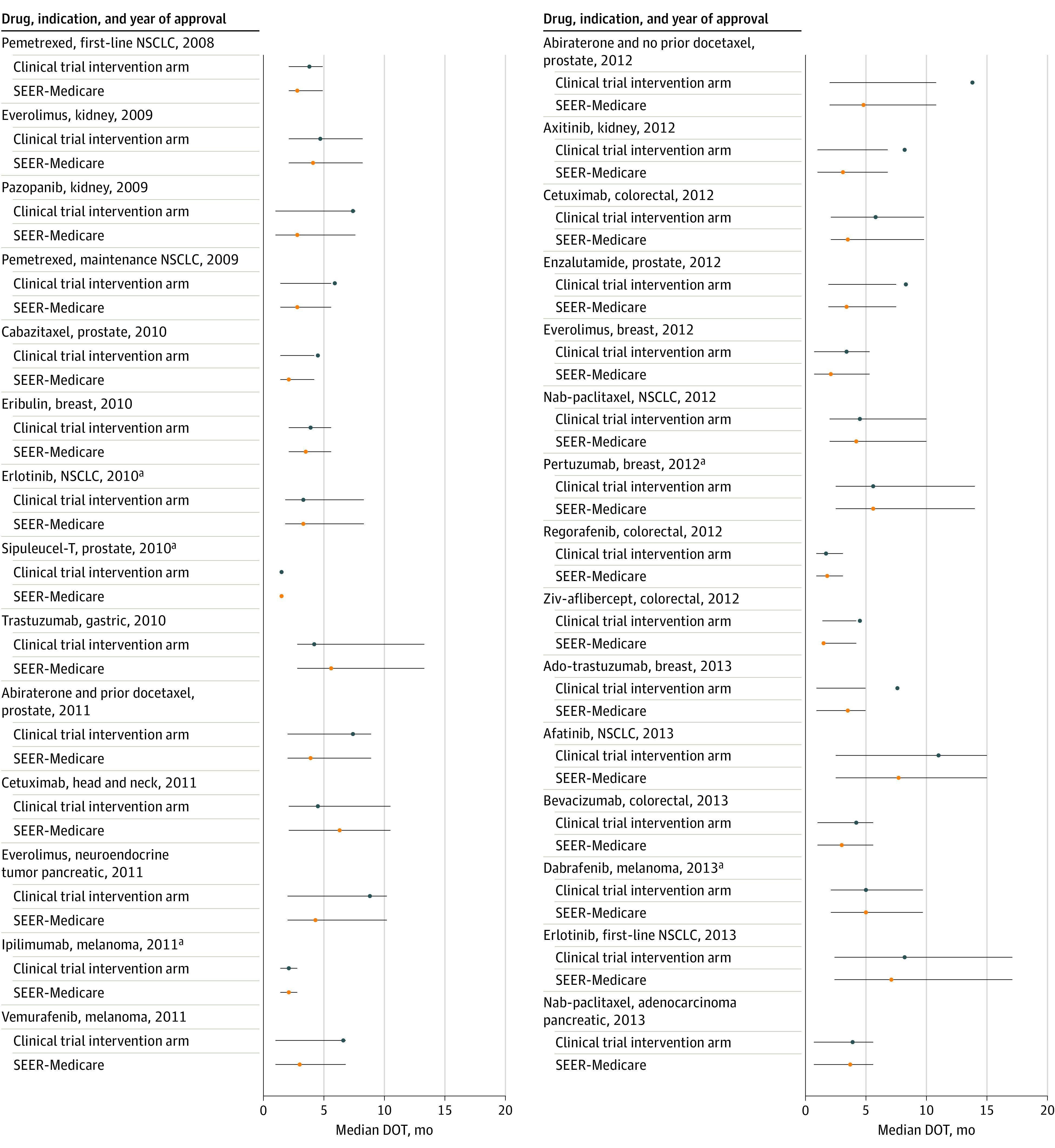
Results: A total of 11 828 trial participants (mean age, 61.8 years; 6718 [56.8%] male; and 7605 [64.3%] White) and 9178 SEER-Medicare patients (mean age, 72.7 years; 4800 [52.3%] male; and 7437 [81.0% White]) were compared. Twenty-nine indications for 22 cancer drugs were included. Median overall survival among Medicare patients was shorter than among patients in the clinical trial intervention arm for 28 of 29 indications (median difference, -6.3 months; range, -28.7 to 2.7 months). Median duration of therapy among Medicare patients was shorter for 23 of the 27 indications with data available (median difference, -1.9 months; range, -12.4 to 1.4 months). For 9 indications, there was information available regarding dose reductions in the package insert or trial publication. In all but 1 instance, dose reductions or single prescriptions were more common in the Medicare population compared with dose reductions among the clinical trial patients; for example, in the Medicare patients, 600 of 1032 (58.1%) received dose reduction or a single prescription and 172 of 1032 (16.7%) received a single prescription vs 734 of 3416 (21.5%) in the trial intervention arm. The exception was afatinib for non-small cell lung cancer: 34 of 71 (47.9%) received dose reduction or a single prescription and 15 of 71 (21.1%) received a single prescription among the Medicare patients vs 120 of 230 (52.2%) receiving dose reductions among the trial intervention group.
Conclusions and relevance: In this cohort study, patients receiving Medicare who were treated with FDA-approved cancer drugs did not live as long as treated clinical trial participants and commonly received treatment modifications. This study suggests that cancer clinical data relevant to newly approved drugs lack generalizability to Medicare beneficiaries with cancer; therefore, these agents should be used with caution.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
