

A Machine Learning Approach to Predict Deep Venous Thrombosis Among Hospitalized Patients
- PMID: 33625875
- PMCID: PMC7907939
- DOI: 10.1177/1076029621991185
A Machine Learning Approach to Predict Deep Venous Thrombosis Among Hospitalized Patients
Abstract
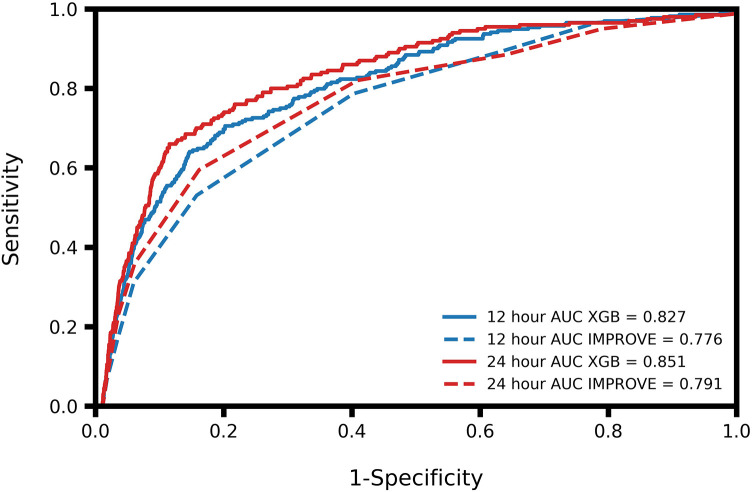
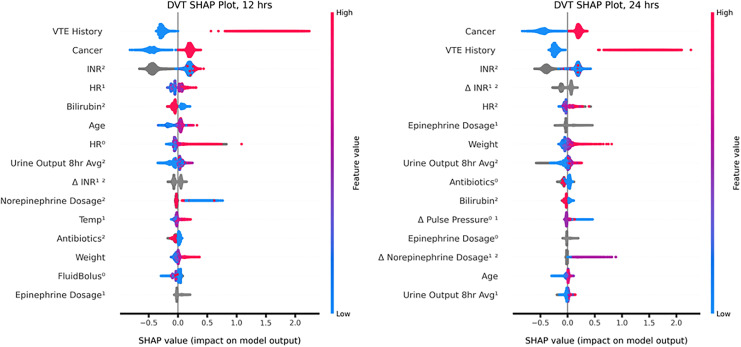
Deep venous thrombosis (DVT) is associated with significant morbidity, mortality, and increased healthcare costs. Standard scoring systems for DVT risk stratification often provide insufficient stratification of hospitalized patients and are unable to accurately predict which inpatients are most likely to present with DVT. There is a continued need for tools which can predict DVT in hospitalized patients. We performed a retrospective study on a database collected from a large academic hospital, comprised of 99,237 total general ward or ICU patients, 2,378 of whom experienced a DVT during their hospital stay. Gradient boosted machine learning algorithms were developed to predict a patient's risk of developing DVT at 12- and 24-hour windows prior to onset. The primary outcome of interest was diagnosis of in-hospital DVT. The machine learning predictors obtained AUROCs of 0.83 and 0.85 for DVT risk prediction on hospitalized patients at 12- and 24-hour windows, respectively. At both 12 and 24 hours before DVT onset, the most important features for prediction of DVT were cancer history, VTE history, and internal normalized ratio (INR). Improved risk stratification may prevent unnecessary invasive testing in patients for whom DVT cannot be ruled out using existing methods. Improved risk stratification may also allow for more targeted use of prophylactic anticoagulants, as well as earlier diagnosis and treatment, preventing the development of pulmonary emboli and other sequelae of DVT.
Keywords: algorithms; deep venous thrombosis; machine learning; risk assessment; venous thromboembolism.
Conflict of interest statement
Figures
Similar articles
-
Risk Stratification Model: Lower-Extremity Ultrasonography for Hospitalized Patients with Suspected Deep Vein Thrombosis.J Gen Intern Med. 2018 Jan;33(1):21-25. doi: 10.1007/s11606-017-4170-3. Epub 2017 Sep 15. J Gen Intern Med. 2018. PMID: 28916935 Free PMC article.
-
Incidence, risk factors, and treatment patterns for deep venous thrombosis in hospitalized children: an increasing population at risk.J Vasc Surg. 2008 Apr;47(4):837-43. doi: 10.1016/j.jvs.2007.11.054. Epub 2008 Mar 4. J Vasc Surg. 2008. PMID: 18295440
-
Inpatient resource use and cost burden of deep vein thrombosis and pulmonary embolism in the United States.Clin Ther. 2015 Jan 1;37(1):62-70. doi: 10.1016/j.clinthera.2014.10.024. Epub 2014 Dec 15. Clin Ther. 2015. PMID: 25524389
-
Development of a risk stratification scoring system for deep vein thrombosis upon psychiatric admission.J Psychosom Res. 2021 Aug;147:110540. doi: 10.1016/j.jpsychores.2021.110540. Epub 2021 May 31. J Psychosom Res. 2021. PMID: 34102544
-
Duplex ultrasound, clinical score, thrombotic risk, and D-dimer testing for evidence based diagnosis and management of deep vein thrombosis and alternative diagnoses in the primary care setting and outpatient ward.Int Angiol. 2014 Feb;33(1):1-19. Int Angiol. 2014. PMID: 24452081 Review.
Cited by
-
Development and validation of a machine learning model to predict venous thromboembolism among hospitalized cancer patients.Asia Pac J Oncol Nurs. 2022 Aug 6;9(12):100128. doi: 10.1016/j.apjon.2022.100128. eCollection 2022 Dec. Asia Pac J Oncol Nurs. 2022. PMID: 36276886 Free PMC article.
-
Chinese experts' consensus on the application of intensive care big data.Front Med (Lausanne). 2024 Jan 8;10:1174429. doi: 10.3389/fmed.2023.1174429. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38264049 Free PMC article.
-
Using machine learning models to predict post-revascularization thrombosis in PAD.Front Artif Intell. 2025 May 7;8:1540503. doi: 10.3389/frai.2025.1540503. eCollection 2025. Front Artif Intell. 2025. PMID: 40400616 Free PMC article.
-
A Broad Learning System to Predict the 28-Day Mortality of Patients Hospitalized with Community-Acquired Pneumonia: A Case-Control Study.Comput Math Methods Med. 2022 Mar 4;2022:7003272. doi: 10.1155/2022/7003272. eCollection 2022. Comput Math Methods Med. 2022. PMID: 35281948 Free PMC article.
-
Machine Learning Approach for Improved Longitudinal Prediction of Progression from Mild Cognitive Impairment to Alzheimer's Disease.Diagnostics (Basel). 2023 Dec 20;14(1):13. doi: 10.3390/diagnostics14010013. Diagnostics (Basel). 2023. PMID: 38201322 Free PMC article.
References
-
- White R H. The epidemiology of venous thromboembolism. Circulation. 2003;107(23_suppl_1):I–4. - PubMed
-
- Mahan CE, Holdsworth MT, Welch SM, Borrego M, Spyropoulos AC. Deep-vein thrombosis: a United States cost model for a preventable and costly adverse event. Thromb Haemost. 2011;106(3):405–415. - PubMed
-
- Kafeza M, Shalhoub J, Salooja N, Bingham L, Spagou K, Davies AH. A systematic review of clinical prediction scores for deep vein thrombosis. Phlebology. 2017;32(8):516–531. - PubMed
-
- Heit JA, Melton LJ, Lohse CM. et al. Incidence of venous thromboembolism in hospitalized patients vs community residents. Mayo Clin Proc. 2001;76(11):1102–1110. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
