

Machine learning-based analysis of alveolar and vascular injury in SARS-CoV-2 acute respiratory failure
- PMID: 33626204
- PMCID: PMC8014445
- DOI: 10.1002/path.5653
Machine learning-based analysis of alveolar and vascular injury in SARS-CoV-2 acute respiratory failure
Abstract
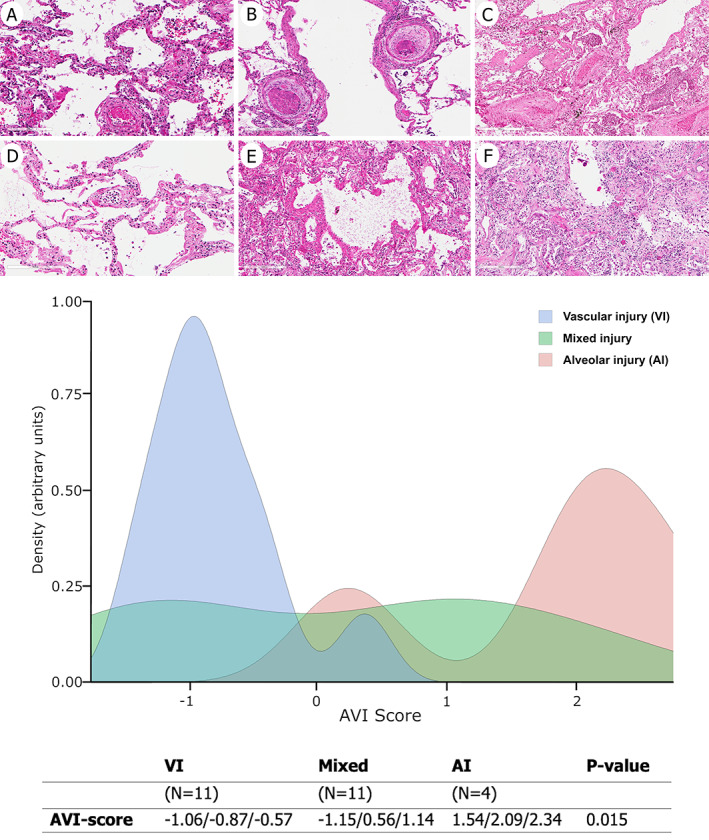
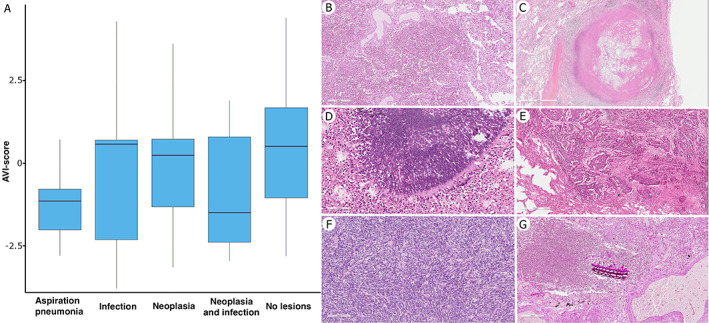
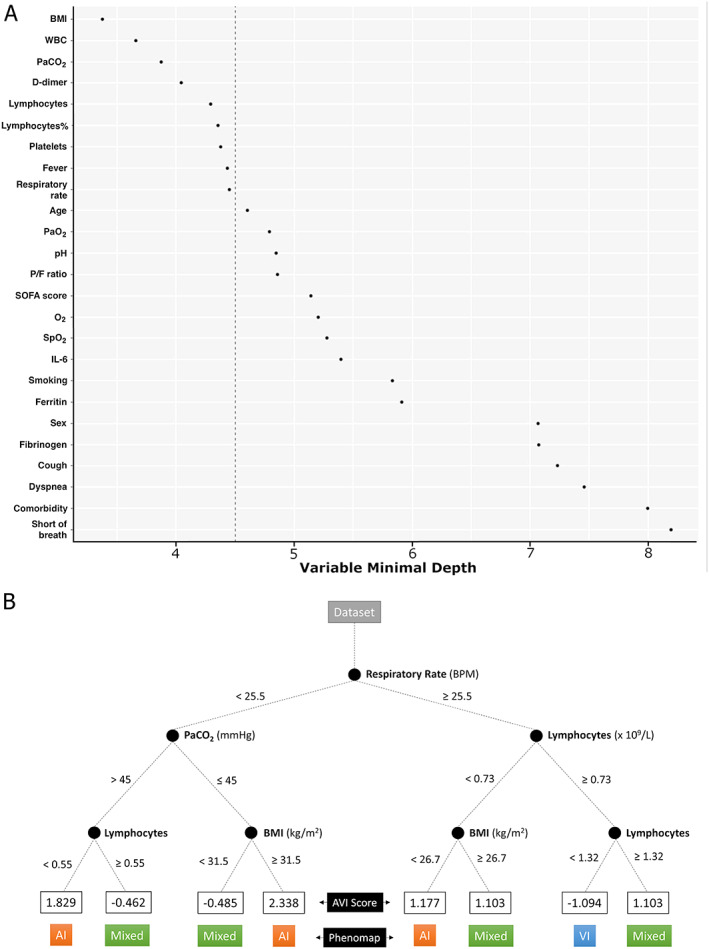
Severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) pneumopathy is characterized by a complex clinical picture and heterogeneous pathological lesions, both involving alveolar and vascular components. The severity and distribution of morphological lesions associated with SARS-CoV-2 and how they relate to clinical, laboratory, and radiological data have not yet been studied systematically. The main goals of the present study were to objectively identify pathological phenotypes and factors that, in addition to SARS-CoV-2, may influence their occurrence. Lungs from 26 patients who died from SARS-CoV-2 acute respiratory failure were comprehensively analysed. Robust machine learning techniques were implemented to obtain a global pathological score to distinguish phenotypes with prevalent vascular or alveolar injury. The score was then analysed to assess its possible correlation with clinical, laboratory, radiological, and tissue viral data. Furthermore, an exploratory random forest algorithm was developed to identify the most discriminative clinical characteristics at hospital admission that might predict pathological phenotypes of SARS-CoV-2. Vascular injury phenotype was observed in most cases being consistently present as pure form or in combination with alveolar injury. Phenotypes with more severe alveolar injury showed significantly more frequent tracheal intubation; longer invasive mechanical ventilation, illness duration, intensive care unit or hospital ward stay; and lower tissue viral quantity (p < 0.001). Furthermore, in this phenotype, superimposed infections, tumours, and aspiration pneumonia were also more frequent (p < 0.001). Random forest algorithm identified some clinical features at admission (body mass index, white blood cells, D-dimer, lymphocyte and platelet counts, fever, respiratory rate, and PaCO2 ) to stratify patients into different clinical clusters and potential pathological phenotypes (a web-app for score assessment has also been developed; https://r-ubesp.dctv.unipd.it/shiny/AVI-Score/). In SARS-CoV-2 positive patients, alveolar injury is often associated with other factors in addition to viral infection. Identifying phenotypical patterns at admission may enable a better stratification of patients, ultimately favouring the most appropriate management. © 2021 The Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Keywords: COVID-19; SARS-CoV-2; acute respiratory failure; alveolar injury; vascular injury.
© 2021 The Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Figures

References
-
- Porcheddu R, Serra C, Kelvin D, et al. Similarity in case fatality rates (CFR) of COVID‐19/SARS‐COV‐2 in Italy and China. J Infect Dev Ctries 2020; 14: 125–128. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
