

Cost-effectiveness analysis of first-line treatments for advanced epidermal growth factor receptor-mutant non-small cell lung cancer patients
- PMID: 33626238
- PMCID: PMC7957173
- DOI: 10.1002/cam4.3733
Cost-effectiveness analysis of first-line treatments for advanced epidermal growth factor receptor-mutant non-small cell lung cancer patients
Abstract
Objectives: Recent studies showed prolonged survival for advanced epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) patients treated with both monotherapies and combined therapies. However, high costs limit clinical applications. Thus, we conducted this cost-effectiveness analysis to explore an optimal first-line treatment for advanced EGFR-mutant NSCLC patients.
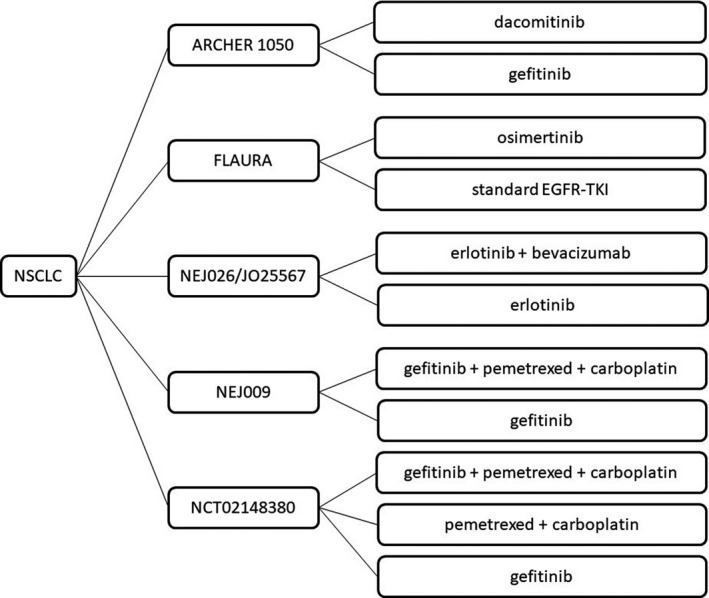
Materials and methods: Survival data were extracted from six clinical trials, including ARCHER1050 (dacomitinib vs. gefitinib); FLAURA (osimertinib vs. gefitinib/erlotinib); JO25567 and NEJ026 (bevacizumab +erlotinib vs. erlotinib); NEJ009 (gefitinib +chemotherapy vs. gefitinib); and NCT02148380 (gefitinib +chemotherapy vs. gefitinib vs. chemotherapy) trials. Cost-related data were obtained from hospitals and published literature. The effect parameter (quality-adjusted life year [QALY]) was the reflection of both survival and utility. Incremental cost-effectiveness ratio (ICER), average cost-effectiveness ratio (ACER), and net benefit were calculated, and the willingness-to-pay (WTP) threshold was set at $30828/QALY from the perspective of the Chinese healthcare system. Sensitivity analysis was performed to explore the stability of results.
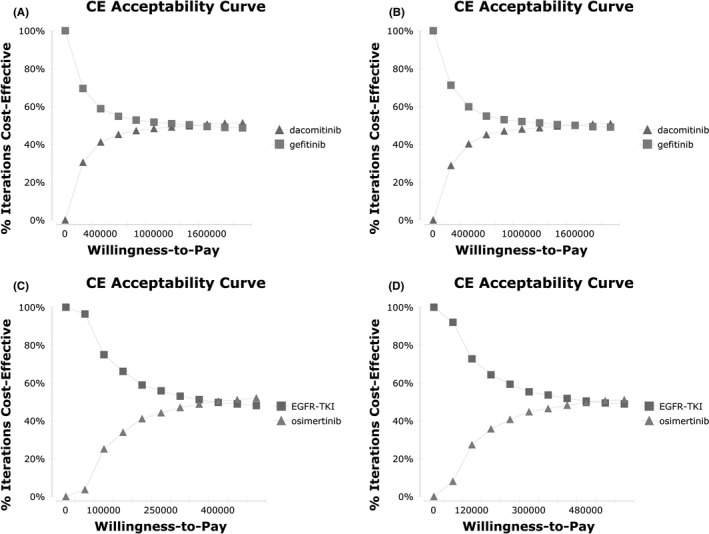
Results: We compared treatment groups with control groups in each trial. ICERs were $1897750.74/QALY (ARCHER1050), $416560.02/QALY (FLAURA), -$477607.48/QALY (JO25567), -$464326.66/QALY (NEJ026), -$277121.22/QALY (NEJ009), -$399360.94/QALY (gefitinib as comparison, NCT02148380), and -$170733.05/QALY (chemotherapy as comparison, NCT02148380). Moreover, ACER and net benefit showed that the combination of EGFR-TKI with chemotherapy and osimertinib was of more economic benefit following first-generation EGFR-TKIs. Sensitivity analyses showed that the impact of utilities and monotherapy could be cost-effective with a 50% cost reduction.
Conclusion: First-generation EGFR-TKI therapy remained the most cost-effective treatment option for advanced EGFR-mutant NSCLC patients. Our results could serve as both a reference for both clinical practice and the formulation of medical insurance reimbursement.
Keywords: cost-effectiveness; epidermal growth factor receptor; first-line therapy; non-small cell lung cancer.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
None.
Figures
Similar articles
-
Cost-effectiveness of Osimertinib as First-line Treatment and Sequential Therapy for EGFR Mutation-positive Non-small Cell Lung Cancer in China.Clin Ther. 2019 Feb;41(2):280-290. doi: 10.1016/j.clinthera.2018.12.007. Epub 2019 Jan 11. Clin Ther. 2019. PMID: 30639208
-
Cost-effectiveness analysis of osimertinib for first-line treatment of locally advanced or metastatic EGFR mutation positive non-small cell lung cancer in Singapore.J Med Econ. 2020 Nov;23(11):1330-1339. doi: 10.1080/13696998.2020.1819822. Epub 2020 Sep 21. J Med Econ. 2020. PMID: 32886557
-
Cost-effectiveness of osimertinib versus standard EGFR-TKI as first-line treatment for locally advanced or metastatic EGFR mutation-positive non-small cell lung cancer in Australia.Expert Rev Pharmacoecon Outcomes Res. 2021 Jun;21(3):415-423. doi: 10.1080/14737167.2021.1847648. Epub 2020 Dec 6. Expert Rev Pharmacoecon Outcomes Res. 2021. PMID: 33151783
-
First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer.Cochrane Database Syst Rev. 2021 Mar 18;3(3):CD010383. doi: 10.1002/14651858.CD010383.pub3. Cochrane Database Syst Rev. 2021. PMID: 33734432 Free PMC article.
-
Cost-effectiveness analysis of the first-line EGFR-TKIs in patients with non-small cell lung cancer harbouring EGFR mutations.Eur J Health Econ. 2020 Feb;21(1):153-164. doi: 10.1007/s10198-019-01117-3. Epub 2019 Sep 20. Eur J Health Econ. 2020. PMID: 31541309 Free PMC article.
Cited by
-
Cost-Effectiveness Analysis of Gefitinib Plus Chemotherapy versus Gefitinib Alone for Advanced Non-Small-Cell Lung Cancer with EGFR Mutations in China.Cancer Manag Res. 2021 Nov 3;13:8297-8306. doi: 10.2147/CMAR.S334643. eCollection 2021. Cancer Manag Res. 2021. PMID: 34764692 Free PMC article.
-
Osimertinib in Patients With Treatment-Naive EGFR-Mutant Non-small Cell Lung Cancer: Overall Survival, Post-progression Management and Budget Impact Analysis in Real-World.Oncologist. 2024 Jul 5;29(7):596-608. doi: 10.1093/oncolo/oyae043. Oncologist. 2024. PMID: 38520745 Free PMC article.
-
Sponsorship bias in published pharmacoeconomic evaluations of national reimbursement negotiation drugs in China: a systematic review.BMJ Glob Health. 2023 Nov 29;8(11):e012780. doi: 10.1136/bmjgh-2023-012780. BMJ Glob Health. 2023. PMID: 38030227 Free PMC article.
-
Optimizing the Treatment for Advanced Non-Small-Cell Lung Cancer with Mutated Epidermal Growth Factor Receptor in Low-Income Countries: A Review.J Immunother Precis Oncol. 2023 Jun 12;6(3):140-149. doi: 10.36401/JIPO-22-29. eCollection 2023 Aug. J Immunother Precis Oncol. 2023. PMID: 37637235 Free PMC article. Review.
-
Panduratin A from Boesenbergia rotunda Effectively Inhibits EGFR/STAT3/Akt Signaling Pathways, Inducing Apoptosis in NSCLC Cells with Wild-Type and T790M Mutations in EGFR.Int J Mol Sci. 2025 Mar 6;26(5):2350. doi: 10.3390/ijms26052350. Int J Mol Sci. 2025. PMID: 40076971 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7‐34. - PubMed
-
- Arbour KC, Riely GJ. Systemic Therapy for Locally Advanced and Metastatic Non‐Small Cell Lung Cancer: A Review. JAMA. 2019;322(8):764‐774. - PubMed
-
- Duma N, Santana‐Davila R, Molina JR. Non‐Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin Proc. 2019;94(8):1623‐1640. - PubMed
-
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD‐3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population‐based registries in 71 countries. Lancet. 2018;391(10125):1023‐1075. - PMC - PubMed
-
- Hsu WH, Yang JC, Mok TS, Loong HH. Overview of current systemic management of EGFR‐mutant NSCLC. Ann Oncol. 2018;29:i3‐i9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
