

Ascertaining Design Requirements for Postoperative Care Transition Interventions
- PMID: 33626584
- PMCID: PMC7904383
- DOI: 10.1055/s-0040-1721780
Ascertaining Design Requirements for Postoperative Care Transition Interventions
Abstract
Background: Handoffs or care transitions from the operating room (OR) to intensive care unit (ICU) are fragmented and vulnerable to communication errors. Although protocols and checklists for standardization help reduce errors, such interventions suffer from limited sustainability. An unexplored aspect is the potential role of developing personalized postoperative transition interventions using artificial intelligence (AI)-generated risks.
Objectives: This study was aimed to (1) identify factors affecting sustainability of handoff standardization, (2) utilize a human-centered approach to develop design ideas and prototyping requirements for a sustainable handoff intervention, and (3) explore the potential role for AI risk assessment during handoffs.
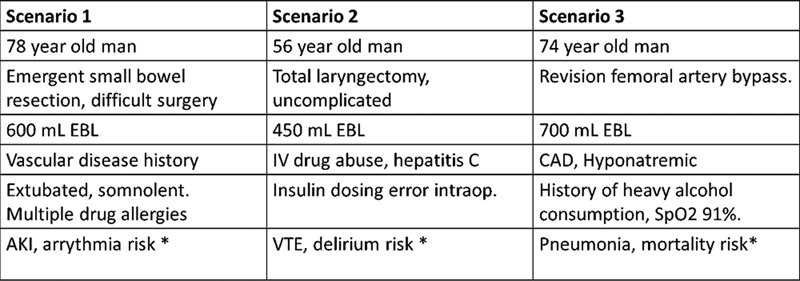
Methods: We conducted four design workshops with 24 participants representing OR and ICU teams at a large medical academic center. Data collection phases were (1) open-ended questions, (2) closed card sorting of handoff information elements, and (3) scenario-based design ideation and prototyping for a handoff intervention. Data were analyzed using thematic analysis. Card sorts were further tallied to characterize handoff information elements as core, flexible, or unnecessary.
Results: Limited protocol awareness among clinicians and lack of an interdisciplinary electronic health record (EHR)-integrated handoff intervention prevented long-term sustainability of handoff standardization. Clinicians argued for a handoff intervention comprised of core elements (included for all patients) and flexible elements (tailored by patient condition and risks). They also identified unnecessary elements that could be omitted during handoffs. Similarities and differences in handoff intervention requirements among physicians and nurses were noted; in particular, clinicians expressed divergent views on the role of AI-generated postoperative risks.
Conclusion: Current postoperative handoff interventions focus largely on standardization of information transfer and handoff processes. Our design approach allowed us to visualize accurate models of user expectations for effective interdisciplinary communication. Insights from this study point toward EHR-integrated, "flexibly standardized" care transition interventions that can automatically generate a patient-centered summary and risk-based report.
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures



References
-
- Nagpal K, Arora S, Abboudi M. Postoperative handover: problems, pitfalls, and prevention of error. Ann Surg. 2010;252(01):171–176. - PubMed
-
- Catchpole K R, de Leval M R, McEwan A. Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Paediatr Anaesth. 2007;17(05):470–478. - PubMed
-
- Agarwal H S, Saville B R, Slayton J M. Standardized postoperative handover process improves outcomes in the intensive care unit: a model for operational sustainability and improved team performance*. Crit Care Med. 2012;40(07):2109–2115. - PubMed
-
- Petrovic M A, Aboumatar H, Baumgartner W A. Pilot implementation of a perioperative protocol to guide operating room-to-intensive care unit patient handoffs. J Cardiothorac Vasc Anesth. 2012;26(01):11–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical