

Remote Hemodynamic-Guided Therapy of Patients With Recurrent Heart Failure Following Cardiac Resynchronization Therapy
- PMID: 33626889
- PMCID: PMC8174266
- DOI: 10.1161/JAHA.120.017619
Remote Hemodynamic-Guided Therapy of Patients With Recurrent Heart Failure Following Cardiac Resynchronization Therapy
Abstract
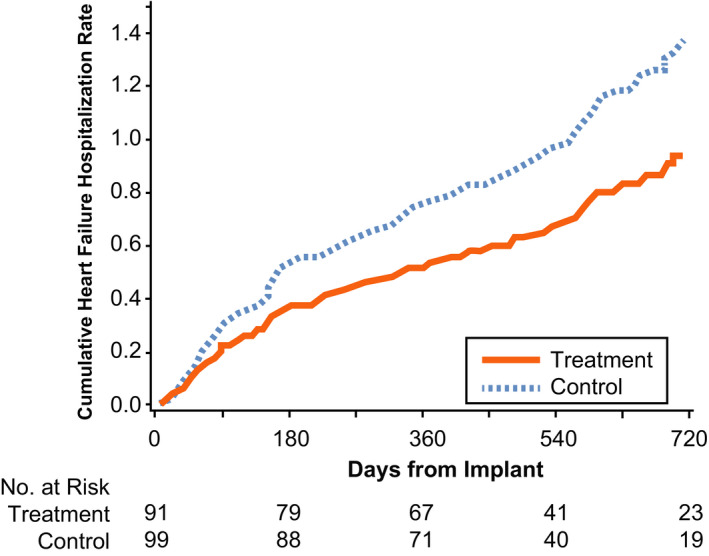
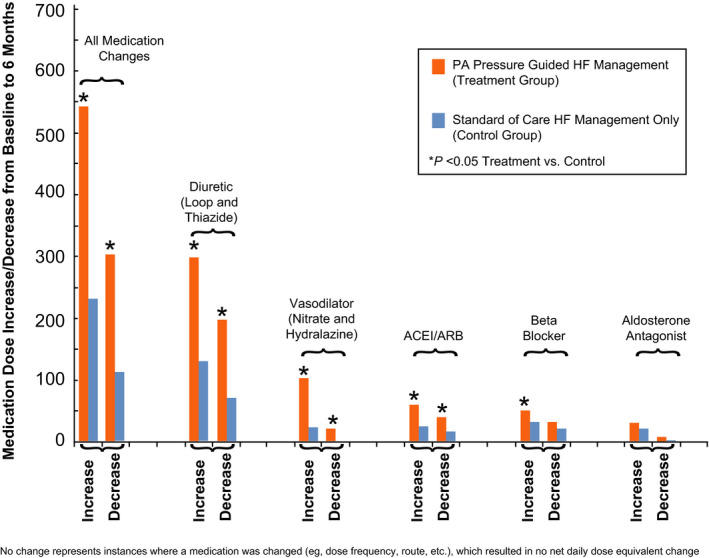
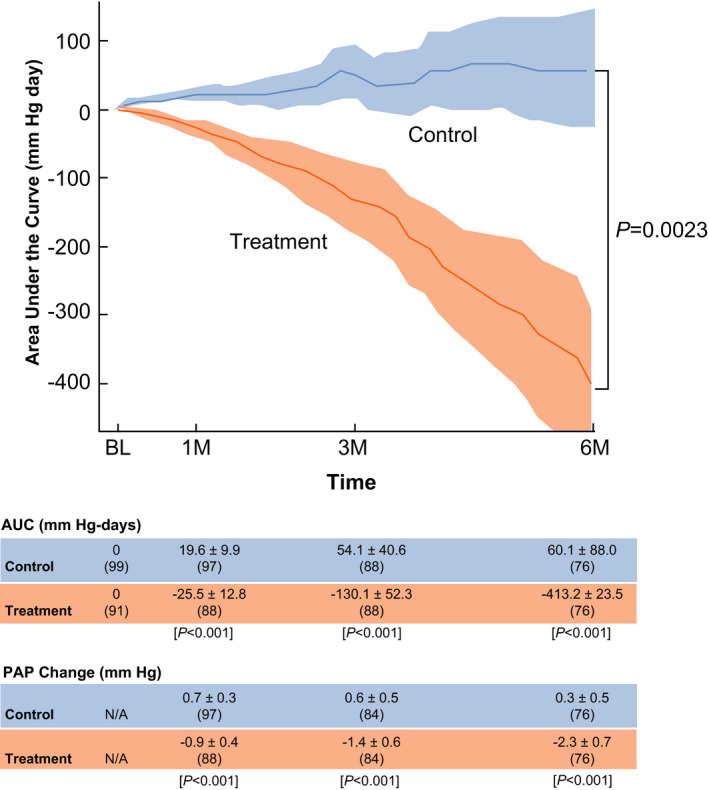
Background Patients with recurring heart failure (HF) following cardiac resynchronization therapy fare poorly. Their management is undecided. We tested remote hemodynamic-guided pharmacotherapy. Methods and Results We evaluated cardiac resynchronization therapy subjects included in the CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in New York Heart Association Class III Heart Failure Patients) trial, which randomized patients with persistent New York Heart Association Class III symptoms and ≥1 HF hospitalization in the previous 12 months to remotely managed pulmonary artery (PA) pressure-guided management (treatment) or usual HF care (control). Diuretics and/or vasodilators were adjusted conventionally in control and included remote PA pressure information in treatment. Annualized HF hospitalization rates, changes in PA pressures over time (analyzed by area under the curve), changes in medications, and quality of life (Minnesota Living with Heart Failure Questionnaire scores) were assessed. Patients who had cardiac resynchronization therapy (n=190, median implant duration 755 days) at enrollment had poor hemodynamic function (cardiac index 2.00±0.59 L/min per m2), high comorbidity burden (67% had secondary pulmonary hypertension, 61% had estimated glomerular filtration rate <60 mL/min per 1.73 m2), and poor Minnesota Living with Heart Failure Questionnaire scores (57±24). During 18 months randomized follow-up, HF hospitalizations were 30% lower in treatment (n=91, 62 events, 0.46 events/patient-year) versus control patients (n=99, 93 events, 0.68 events/patient-year) (hazard ratio, 0.70; 95% CI, 0.51-0.96; P=0.028). Treatment patients had more medication up-/down-titrations (847 versus 346 in control, P<0.001), mean PA pressure reduction (area under the curve -413.2±123.5 versus 60.1±88.0 in control, P=0.002), and quality of life improvement (Minnesota Living with Heart Failure Questionnaire decreased -13.5±23 versus -4.9±24.8 in control, P=0.006). Conclusions Remote hemodynamic-guided adjustment of medical therapies decreased PA pressures and the burden of HF symptoms and hospitalizations in patients with recurring Class III HF and hospitalizations, beyond the effect of cardiac resynchronization therapy. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT00531661.
Keywords: cardiac resynchronization therapy; heart failure; hemodynamic; hemodynamic monitoring; pulmonary artery pressure; remote monitoring.
Conflict of interest statement
Niraj Varma reports consulting Fees/Honoraria from St. Jude Medical, Boston Scientific, Biotronik, Medtronic. Robert Bourge reports grant support and consulting fees from Abbott (CardioMEMS). Lynne Stevenson is an unpaid consultant for Abbott and Biotronik and Chair of the DSMB for LivaNova. Mariarosa Rosa Costanzo reports consulting Fees/Honoraria from Abbott, Medtronic, Boston Scientific, and grant support from Abbott to the Advocate Heart Institute for the CardioMEMS postapproval study and GUIDE‐HF clinical trial. Philip B. Adamson reports salary support from Abbott. Greg Ginn reports salary support from Abbott. John Henderson reports salary support from Abbott. David Shavelle reports grant support from Abbott for CardioMEMS clinical trials.
Figures
Comment in
-
Is Ambulatory Hemodynamic Monitoring Beneficial to Patients With Advanced Heart Failure?J Am Heart Assoc. 2021 Feb;10(5):e020817. doi: 10.1161/JAHA.121.020817. Epub 2021 Feb 25. J Am Heart Assoc. 2021. PMID: 33626878 Free PMC article. No abstract available.
Similar articles
-
Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmonary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes From the CardioMEMS Post-Approval Study.Circ Heart Fail. 2020 Aug;13(8):e006863. doi: 10.1161/CIRCHEARTFAILURE.119.006863. Epub 2020 Aug 6. Circ Heart Fail. 2020. PMID: 32757642 Free PMC article.
-
Interventions Linked to Decreased Heart Failure Hospitalizations During Ambulatory Pulmonary Artery Pressure Monitoring.JACC Heart Fail. 2016 May;4(5):333-44. doi: 10.1016/j.jchf.2015.11.011. Epub 2016 Feb 10. JACC Heart Fail. 2016. PMID: 26874388
-
Remote Hemodynamic Monitoring Equally Reduces Heart Failure Hospitalizations in Women and Men in Clinical Practice: A Sex-Specific Analysis of the CardioMEMS Post-Approval Study.Circ Heart Fail. 2021 Jun;14(6):e007892. doi: 10.1161/CIRCHEARTFAILURE.120.007892. Epub 2021 Jun 15. Circ Heart Fail. 2021. PMID: 34129363
-
Current Role of the CardioMEMS Device for Management of Patients with Heart Failure.Curr Cardiol Rep. 2019 Jul 27;21(9):98. doi: 10.1007/s11886-019-1194-9. Curr Cardiol Rep. 2019. PMID: 31352531 Review.
-
Remote monitoring: Doomed to let down or an attractive promise?Int J Cardiol Heart Vasc. 2019 May 30;24:100380. doi: 10.1016/j.ijcha.2019.100380. eCollection 2019 Sep. Int J Cardiol Heart Vasc. 2019. PMID: 31193998 Free PMC article. Review.
Cited by
-
Is Ambulatory Hemodynamic Monitoring Beneficial to Patients With Advanced Heart Failure?J Am Heart Assoc. 2021 Feb;10(5):e020817. doi: 10.1161/JAHA.121.020817. Epub 2021 Feb 25. J Am Heart Assoc. 2021. PMID: 33626878 Free PMC article. No abstract available.
-
Can Right Heart Catheterization Improve the Prediction of Positive Response to Resynchronization Therapy?Biomedicines. 2025 Feb 14;13(2):467. doi: 10.3390/biomedicines13020467. Biomedicines. 2025. PMID: 40002881 Free PMC article.
-
2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure.J Arrhythm. 2023 Aug 2;39(5):681-756. doi: 10.1002/joa3.12872. eCollection 2023 Oct. J Arrhythm. 2023. PMID: 37799799 Free PMC article.
-
Do the Current Guidelines for Heart Failure Diagnosis and Treatment Fit with Clinical Complexity?J Clin Med. 2022 Feb 6;11(3):857. doi: 10.3390/jcm11030857. J Clin Med. 2022. PMID: 35160308 Free PMC article. Review.
-
Digital Transformation in the Diagnostics and Therapy of Cardiovascular Diseases: Comprehensive Literature Review.JMIR Cardio. 2023 Aug 30;7:e44983. doi: 10.2196/44983. JMIR Cardio. 2023. PMID: 37647103 Free PMC article. Review.
References
-
- Anand IS, Carson P, Galle E, Song R, Boehmer J, Ghali JK, Jaski B, Lindenfeld J, O'Connor C, Steinberg JS, et al. Cardiac resynchronization therapy reduces the risk of hospitalizations in patients with advanced heart failure: results from the comparison of medical therapy, pacing and defibrillation in heart failure (COMPANION) trial. Circulation. 2009;119:969–977. - PubMed
-
- Rickard J, Cheng A, Spragg D, Bansal S, Niebauer M, Baranowski B, Cantillon DJ, Tchou PJ, Grimm RA, Tang WH, et al. Durability of the survival effect of cardiac resynchronization therapy by level of left ventricular functional improvement: fate of "nonresponders". Heart Rhythm. 2014;11:412–416. - PubMed
-
- Varma N, Boehmer J, Bhargava K, Yoo D, Leonelli F, Costanzo M, Saxena A, Sun L, Gold MR, Singh J, et al. Evaluation, management, and outcomes of patients poorly responsive to cardiac resynchronization device therapy. J Am Coll Cardiol. 2019;74:2588–2603. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
