

Diagnosis and surgical treatment of primary isolated aggressive lumbar myeloid sarcoma: a rare case report and review of the literatures
- PMID: 33627110
- PMCID: PMC7905608
- DOI: 10.1186/s12891-021-04066-2
Diagnosis and surgical treatment of primary isolated aggressive lumbar myeloid sarcoma: a rare case report and review of the literatures
Abstract
Background: Myeloid sarcoma is a rare, extramedullary, solid tumor derived from immature myeloid cell precursors. It is most frequently accompanied by acute myelogenous leukemia, though infrequently found in non-acute myelogenous leukemia patients. The tumor may involve any part of the body, but the lumbar spine is seldom involved. The present case study aims to understand the diagnosis and surgical treatment of a rare primary isolated myeloid sarcoma of the lumbar spine causing aggressive spinal cord compression in a non-acute myelogenous leukemia patient.
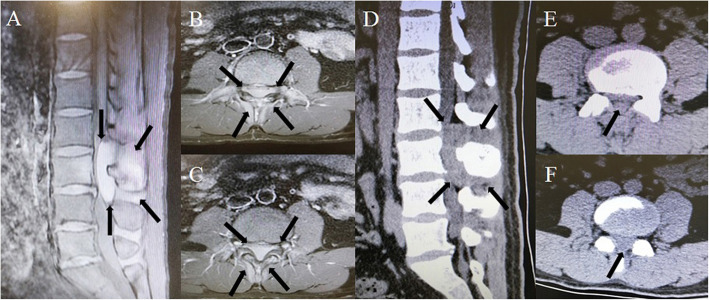
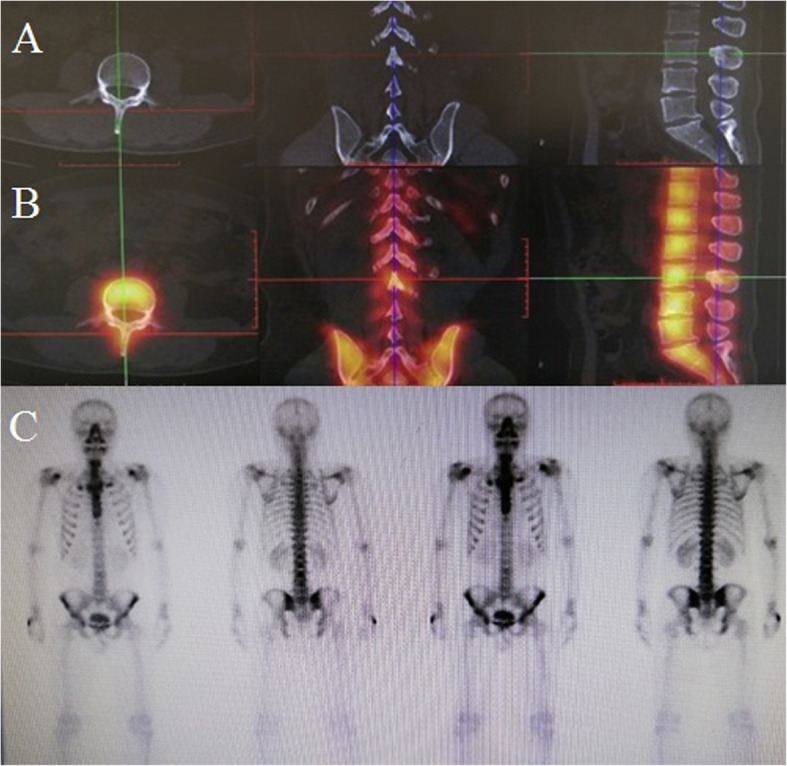
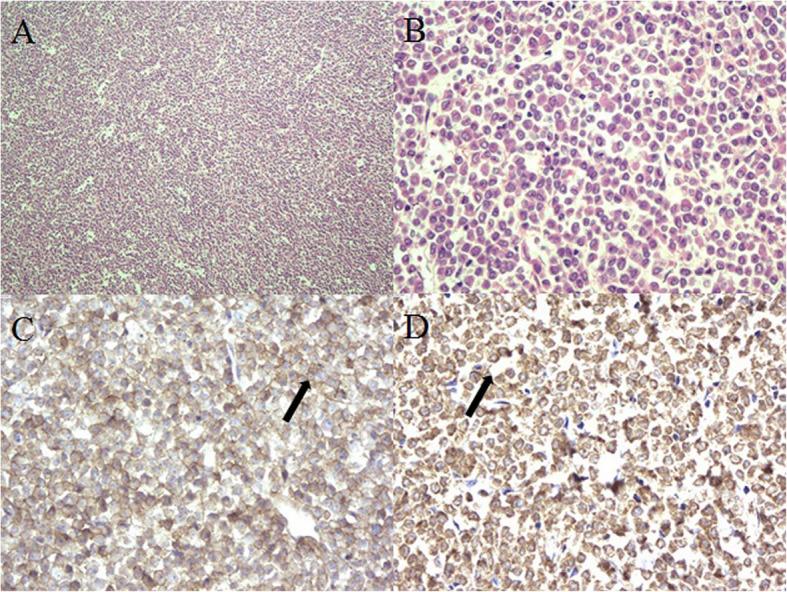
Case presentation: A 29-year-old man complained of an aggressive radiating pain to the lower extremities and moderate dysuria with a Visual Analogue Scale score that gradually increased from 3 to 8. Lumbar enhanced magnetic resonance imaging and computed tomography revealed a lumbar canal lesion at lumbar spine L2 to L4 with spinal cord compression. A whole body bone scan with fused single photon emission computed tomography/computed tomography demonstrated abnormal 99mTc-methylene diphosphonate accumulation in the L3 lamina and spinous process. No evidence of infection or hematology disease was observed in laboratory tests. Due to rapid progression of the symptoms and lack of a clear diagnosis, decompression surgery was performed immediately. During the operation, an approximately 6.0 × 2.5 × 1.2 cm monolithic, fusiform, soft mass in the epidural space and associated lesion tissues were completely resected. The radiating pain was relieved immediately and the dysuria disappeared within 1 week. Intraoperative pathological frozen section analysis revealed a hematopoietic malignant tumor and postoperative immunohistochemistry examination confirmed the diagnosis of myeloid sarcoma.
Conclusions: The primary isolated aggressive lumbar myeloid sarcoma is rarely seen, the specific symptoms and related medical history are unclear. Surgery and hematological treatment are effective for understanding and recognizing this rare tumor.
Keywords: Acute myelogenous leukemia; Case report; Decompression surgery; Lumbar spine; Myeloid sarcoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Aggressive Myeloid Sarcoma Causing Recurrent Spinal Cord Compression.World Neurosurg. 2015 Sep;84(3):866.e7-10. doi: 10.1016/j.wneu.2015.04.017. Epub 2015 Apr 15. World Neurosurg. 2015. PMID: 25888811
-
Spinal granulocytic sarcoma (chloroma) presenting as acute cord compression in a nonleukemic patient.Neurol India. 2005 Jun;53(2):221-3. doi: 10.4103/0028-3886.16418. Neurol India. 2005. PMID: 16010065
-
Granulocytic sarcoma: an unusual complication of aleukemic myeloid leukemia causing spinal cord compression. A case report and literature review.Leuk Lymphoma. 2003 Oct;44(10):1753-60. doi: 10.1080/1042819031000104051. Leuk Lymphoma. 2003. PMID: 14692530 Review.
-
Epidural Spinal Cord Compression as the Presenting Manifestation of Acute Myeloid Leukemia: A Case Report and Literature Review.Intern Med. 2023 Feb 1;62(3):453-457. doi: 10.2169/internalmedicine.9580-22. Epub 2022 Jul 5. Intern Med. 2023. PMID: 35793962 Free PMC article. Review.
-
Myeloid sarcoma with multiple lesions of the central nervous system in a patient without leukemia. Case report.J Neurosurg. 2006 Dec;105(6):916-9. doi: 10.3171/jns.2006.105.6.916. J Neurosurg. 2006. PMID: 17405266
Cited by
-
Clinical characteristics, treatment, and prognosis of 118 cases of myeloid sarcoma.Sci Rep. 2022 Apr 26;12(1):6752. doi: 10.1038/s41598-022-10831-7. Sci Rep. 2022. PMID: 35474239 Free PMC article.
-
Myeloid sarcoma with ulnar nerve entrapment: A case report.World J Clin Cases. 2022 Oct 6;10(28):10227-10235. doi: 10.12998/wjcc.v10.i28.10227. World J Clin Cases. 2022. PMID: 36246824 Free PMC article.
-
A rare case of spinal myeloid sarcoma.Surg Neurol Int. 2024 Nov 15;15:415. doi: 10.25259/SNI_640_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39640355 Free PMC article.
-
Spinal Cord Compression As the Initial Manifestation of Relapsed Acute Myeloid Leukemia: A Case Report and Literature Review of a Rare Presentation.Cureus. 2025 Mar 31;17(3):e81509. doi: 10.7759/cureus.81509. eCollection 2025 Mar. Cureus. 2025. PMID: 40308387 Free PMC article.
-
Myeloid sarcoma of the thoracic spine: A case report.Surg Neurol Int. 2023 Jan 27;14:35. doi: 10.25259/SNI_1167_2022. eCollection 2023. Surg Neurol Int. 2023. PMID: 36895207 Free PMC article.
References
-
- Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M, Piccaluga PP, Agostinelli C, Asioli S, Novero D, Bisceglia M, Ponzoni M, Gentile A, Rinaldi P, Franco V, Vincelli D, Pileri A, Jr, Gasbarra R, Falini B, Zinzani PL, Baccarani M. Myeloid sarcoma:clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia. 2007;21(2):340–350. doi: 10.1038/sj.leu.2404491. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
